Introduction
According to epidemiological data, diseases of the musculoskeletal system all over the world are considered to be one of the most common medical and social problems of modern society. Thus, 10–20 % of the world’s population suffers from musculoskeletal diseases, which belongs to a heterogeneous group of diseases of various etiologies, while in 10 % of the cases there is a persistent disability and deterioration in the quality of life due to severe pain and limitation of normal motor activity [1].
During pregnancy, from 33 to 50 % of women report pain in the lumbar spine up to 20 weeks of pregnancy, and over time, the prevalence of pain reaches 60–70 % [2]. Pain syndrome is caused by instability of the joints of the spine and pelvic joints, dyscalgia, functional blockade of the motor segments of the lumbar spine, as well as symphysitis. The main reasons for these changes are either existing chronic diseases of the musculoskeletal system or accompanying osteoporosis, diastasis of the rectus abdominis muscles, and dysfunction of the pelvic floor muscles [3].
In accordance with epidemiological studies, women are more susceptible to musculoskeletal and rheumatic diseases [4]. Gender, age, lipid disorders, previous joint trauma, genetic predisposition, infectious agents, epigenetic and mechanical factors are the most common risk factors for di–seases of the musculoskeletal system [5, 6].
Vitamin D deficiency (VDD) is a global health problem all over the world and the significance of its pleiotropic effects in the pathogenetic mechanisms of cardiovascular, oncological, and dermatological diseases, in the development of diabetes, metabolic syndrome, pregnancy and childbirth complications has a large information base nowadays. There is a lot of information about genetic regulation of its influence. During pregnancy, VDD in the mother, in addition to the regulation of calcium homeostasis, congenital rickets and fractures in newborns is associated with the development of preeclampsia, gestational diabetes, preterm birth, fetal growth retardation, and its prescription improves perinatal outcomes [7–10].
The modern trend to plan pregnancy at a mature age after social development has led to an increase in the incidence of diseases of the musculoskeletal system during pregnancy and in the postpartum period [11, 12]. According to Yucesoy B. (2015), numerous studies have shown the influence of genetic variability on the pathogenesis of diseases of the musculoskeletal system. Genetic variants of several groups of genes, such as the structural genes of the extracellular matrix of cartilage and genes associated with bone tissue density are involved in the pathogenesis of the disease [13]. There is data about the direct relationship between the frequency of lumbar spine pathology and Bsml, Apal, and Taql polymorphisms of the gene encoding vitamin D receptor (VDR), which may be a promising direction for a personalized approach in identifying genetic risk factors, forecasting, and carrying out preventive measures in a specific group of the patients [14, 15].
There is evidence that the musculoskeletal system disea–ses in pregnant women are associated with negative perinatal consequences (preeclampsia, premature birth, fetal growth retardation, postpartum hemorrhage, etc.) [16, 17].
Due to the relevance and multifactorial genesis of di–seases of the musculoskeletal system, and the importance of skeletal and extra-skeletal effects of calcitriol during pregnancy and childbirth, the aim of the research was to determine the incidence of musculoskeletal diseases in pregnant women at high infection risk (HIR) with impaired vitamin D (VD) status and single-nucleotide Bsml (rs1544410) polymorphism of the gene encoding vitamin D receptors.
Materials and methods
Population
From September 2018 to September 2019, 96 pregnant women had been examined at the Maternity Hospitals 5 and 1 in Odesa, which are clinical bases of the Odessa National Medical University (ONMedU). The control group consisted of 40 women with a physiological course of pregnancy and the absence of any indices of the risks of intrauterine infection, and the main group included 56 pregnant women with HIR. The examination of pregnant women was carried out in the period from 24 to 34 weeks of gestation.
The study was approved by the commission on bioethics of ONMedU (protocol No. 124 dated 02.02.2018) and was conducted in accordance with the requirements of the Declaration of Helsinki after the women had signed informed voluntary consent to participate in the study. The work was part of the scientific topic of the Department of Obstetrics and Gynecology of Odessa National Medical University “Improving methods of prevention, diagnosis and treatment of diseases of the female reproductive system using the latest medical molecular genetic technologies”, registration number 0117 U007494.
The criteria for inclusion in the study were and pregnancy with a HIR and age from 18 to 40 years to exclude the influence on the level of VD of factors of formation or reduction of bone tissue mass.
Pregnant women with severe extragenital pathology (diabetes mellitus, chronic diseases of kidneys and liver with failure), with disorders of fat metabolism, skin and autoimmune diseases in the active phase, thyroid and parathyroid gland diseases were excluded from the study.
Methods
A high risk of perinatal infection was determined on the basis of bacterioscopic/bacteriological, serological, ELISA, and PCR studies for the presence of infectious agents that are the causative agents of inflammatory diseases of the urogenital tract and TORCH infections (toxoplasmosis, –others — hepatitis B, coxsackie viruses, syphilis, HIV infection, chlamydia, parvovirus B19 etc. infection, all sexually transmitted diseases, rubella, сytomegalovirus, herpes simplex infection). The criterion for the risk of infection directly in the urogenital tract was the selection of opportunistic/pathogenic microflora in the amount of 105 CFU/ml or more; the diagnosis of TORCH-infections was based on the determining the dynamics of immunoglobulins of the G/M class (IgG, IgM) in the blood, with the detection of antibody avidity. The presence in the anamnesis of chronic inflammatory diseases of the gastrointestinal tract, urinary system, kidneys, ARVI during the pregnancy was taken into account.
General clinical examination of pregnant women was carried out in accordance with the requirements of the regulatory documents of the Ministry of Health of Ukraine.
Clinical signs of perinatal infection included a set of changes detected during ultrasound examination of the placenta, amnion, and fetus (oligohydramnios, hypertrophy, calcinosis, premature maturation of the placenta, fetal ventriculomegaly, and ultrasound signs of hyperechoic intestine).
Diagnosis of the presence of the concomitant extragenital diseases, including of the musculoskeletal system was based on the anamnesis, expert opinions, and the results of studies (X-ray, computer tomography, magnetic resonance imaging), which were performed before pregnancy.
The concentration of 25(OH)D in the blood of pregnant women was determined by the solid-phase ELISA method, based on the principle of competitive binding, on the Cobas Integra analyzer 400 Plus (Roche Diagnostics, Switzerland). Assessment of VD availability was carried out in accordance with Methodological recommendations for the treatment and prevention of VDD for the population of Central European countries (2022), Conclusion of the American College of Obstetricians and Gynecologists Committee (No. 495, 2021), according to which a VD level in blood serum below 20 ng/ml
indicates its deficiency, 20–30 ng/ml — VD insufficiency, VD level more than 30 and 50 ng/ml is considered optimal.
Real-time polymerase chain reaction (PCR) was used to detect the Bsml mutant variant (rs1544410) polymorphism of the gene encoding VDR receptors. Forward and reverse primers (F5’-ACCAAGACTACAAGTACCGCGTCA-3’ and R5’-CTCCCTCTTCCACCTCTAACCAGC-3’) were used for amplification using a DT-96 detection amplifier (NVO DNA-Technology LLC, Russia). The reagent of DNA-Technology company “Proba-Rapid-Genetics” was used for DNA isolation by an express method. The molecular genetic studies were carried out on the basis of the Diagnostic Center “Evgenika” in Odesa.
Statistical analysis
Statistical processing of the results was carried out by creating a database using MS Excel software and the online resource www.socscistatistics.com. The normality of the distribution of these variation series was determined using the Shapiro-Wilk test; to compare quantitative indices under the condition of normal distribution, the Student’s t-test and the non-parametric Mann-Whitney U test were used for data with non-normal distribution. The significance of the results of quality indices was determined using Fisher’s test. The statistical significance of frequency indices, namely the distribution of different alleles and genotypes in groups of the patients, was determined by calculating the odds ratio (OR) using a 95% confidence interval (CI).
Results
According to age and anthropometric indices, the stu–died groups were homogeneous. The average age of pregnant women in the main group was 29.2 ± 4.3 years, and in the control group — 30.40 ± 3.12 years (Uemp = 958; p = 0.30). Body mass index (BMI) in the patients of the main group corresponded to 22.2 ± 1.7 kg/m2, and in the control group — 22.8 ± 1.9 kg/m2 (Uemp = 1066; p = 0.34). In the main group, the number of women giving birth for the first time, was greater than in the control group (40 persons (71.4 %) versus 22 subjects (55.0 %); F = 0.13; p = 0.13).
The presence of diseases of the musculoskeletal system was indicated by 32.1 % (18 women) and 12.5 % (5 women) of the main and control groups, respectively (OR = 3.149; 95% CI: 1.54–6.46). It should be noted that all women with the musculoskeletal system diseases had complaints of recurrent pain in one or another part of the spine or pelvic bones, pain in the lower back, back, hand, wrist, and hips.
Other pathology, in particular, the chronic gastrointestinal tract diseases (gastritis, gallstone pancreatitis) was observed in 3 persons (5.5 %) and 1 person (2.5 %) of pregnant wo–men, respectively, in the main and control groups (F = 0.64; p = 0.64). 37.5 % (21 females) and 15 % (6 women) from groups I and II were diagnosed with chronic pyelonephritis (F = 0.02; p = 0.02); 14.29 % (3 females) of them had an exacerbation of the disease during pregnancy. In the main group, the incidence of ARVI was probably higher (17 wo–men (30.4 %) vs. 3 females (7.5 %); F = 0.0096; p = 0.01).
In pregnant women of the main group, polyhydramnios (12 women (21.4 %) vs. 3 females (7.5 %); F = 0.09; p = 0.09) was noted 2.8 times more often, and oligohydramnios (22 women (39.3 %) and 2 females (5.0 %); F = 0.0001; p = 0.0001) — almost 8 times more often. Violation of placentation (low placentation) was diagnosed in 26.79 % (15 persons) of pregnant women of the main group and 7.5 % (3 persons) of the control group (F = 0.02; p = 0.02); hypertrophy of the placenta was observed in 10.71 % (6 women) and 2.5 % (1 female), respectively (F = 0.23; p = 0.23). The specified ultrasound criteria are signs of inflammatory changes in extraembryonic formations. Ventriculomegaly in the fetus in 12.5 % (7 subjects) of pregnant women also indicated perinatal infection in the main group; there was no such pathology among the patients of the control group (F = 0.039; p = 0.04). Signs of the hyperechoic intestine of the intrauterine fetus were detected only in 10.71 % (6 persons) of pregnant women of the main group during the ultrasound examination (F = 0.039; p = 0.04).
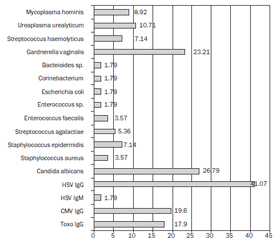
The results of the evaluation of urogenital microflora and examination for TORCH infection which reflect the pre–sence of infectious agents of viral and bacterial origin, are presented in Fig. 1.
The study of the level of 25(OH)D in blood serum revealed significantly worse indices of the VD status in pregnant women with HIR compared to females with a physio–logical course of pregnancy (Fig. 2).
In 76.8 % (43 subjects) of pregnant women of the main group the VD level was lower than optimal (below 30 ng/ml), and in the control group the number of the females with VD deficiency and VD insufficiency was only 15 % (16 women) (F = 0.0003; p = 0.0003) (Fig. 3).
The following frequency of distribution of genotypes and alleles of the Bsml polymorphism (rs1544410) of the gene encoding VDR was found among the examined groups of pregnant women based on the results of molecular genetic testing (Fig. 4).
There was no significant difference in the number of women with the A/A genotype in the main (12.5 % — 7 wo–men) and control (17.5 % — 7 females) groups (OR = 0.68; 95% CI: 0.31–1.48; χ2 = 1.01, р = 0.61). Among pregnant women with HIR, homozygous carriage of the G (guanine) allele (G/G) was observed in 11 women (19.64 %), in contrast to healthy pregnant females, in whom this index was 47.50 % (19 women) (OR = 0.27; 95% CI: 0.15–0.51; χ2 = 16.71, p = 0.00006). A heterozygous combination of A/G alleles was noted in 67.9 and 35 % of women in the groups with HIR and healthy pregnant women, respectively (OR = 3.95; 95% CI: 2.19–7.1; χ2 = 20.88, p = 0.00001).
As mentioned, 32.14 % (18 subjects) from the group with HIR pregnant women indicated diseases of the musculoskeletal system, while in compared group the number of such females was 12.5 % (5 women; OR = 3.15; 95% CI: 1.54–6.46).
The study of the Bsml polymorphism gene encoding VDR showed that 71.4 % (13 subjects) of pregnant women with HIR and 20 % (1 person) of healthy pregnant woman who indicated diseases of the musculoskeletal system, were carriers of the A/G polymorphic allele (OR = 9.79; 95% CI: 5.10–18.82); 28.6 % (5 women) and 60 % (3 females), respectively, were carriers of the homozygous A/A allele (OR = 0.27; 95% CI: 0.15–0.49), and the G/G genotype was typical for only 1 pregnant woman among healthy females (OR = 0.04; 95% CI: 0.005–0.308).
Discussion
As it was mentioned, the examined pregnant women were homogeneous in terms of age and anthropometric characteristics, which excludes the influence of the specified known risk factors on the frequency of joint diseases in these women.
Diseases of the musculoskeletal system, in general, in the anamnesis in pregnant women with HIR were 2.6 times more frequent (in 18 out of 56 subjects) than in healthy pregnant females; including reactive arthritis (in a 33.3 %) of these 18 wo–men. The presence of HIR in pregnant women can lead to a complicated course of pregnancy and a negative outcome of childbirth, and diseases of the musculoskeletal system can also play a certain negative role in the course and outcomes of pregnancy. On the other hand, the viral-bacterial associations, namely the carriage of herpes virus (41.1 %) and cytomegalovirus (19.6 %) infections, as well as toxoplasmosis (17.9 %), which we have found out, can affect, in some way, the bone tissue and the joints. The influence of an infectious agent on the development of reactive arthritis is a known factor [6, 18]. Taking into account that the confirmation of joint diseases in the patients was based exclusively on the anamnesis data, the results of the examination and the conclusions of specialists before the pregnancy, it is possible that the presence of chronic diseases of the urinary tract (37.5 %) and the gastrointestinal tract (5.5 %) could also be one of the factors that contributed to the development of, most likely, reactive damage to the joints. According to the literature, reactive arthritis is an immune-mediated syndrome, which is provoked by a recent infection. It is expected that bacterial fragments (lipopolysaccharides and nucleic acids) reach the systemic circulation, induce T lymphocytes, and then these activated cytotoxic T cells attack the synovium and other self-antigens through molecular mimicry. This is confirmed by the presence of ribosomal RNA transcripts of Chlamydia trachomatis and C.pneumoniae, intestinal bacterial DNA and products of bacterial breakdown in synovial tissue and fluid. In reactive arthritis, the synthesis of anti-inflammatory cytokines is also disrupted, which leads to a decrease in the elimination of bacteria [19]. It is quite likely that a certain role in the genesis of chronic persistent infection in this group of pregnant women can be played by the deficiency of vitamin D, which we have discovered during the research. Among the conditionally pathogenic flora that we identified during the bacteriological examination of urogenital secretions, the most frequently identified were Staphylococcus aureus, Bacteroides sp., Streptococcus haemolyticus (each 7.14 %), Streptococcus agalactiae (5.36 %). Special attention is paid to the latter in the genesis of chronic inflammatory diseases, including those of the bone and joint system. In general, in the development of inflammatory and dege–nerative joint diseases, including of an autoimmune nature, attention is paid to the influence of exo- and endogenous factors, which include lifestyle, bad habits, infection with viral-bacterial associations, genetic features, etc. [19].
The presence of VDR in immunocompetent cells determines the stimulation of 1,25(OH)2D formation by interfe–ron γ, Toll-like receptors after their interaction with lipopolysaccharides, lipoproteins and other molecular components of microorganisms. Subsequently, 1,25(OH)2D stimulates the synthesis of cathelicidin and β-defensin, which are antimicrobial peptides and have a pronounced inhibitory effect on bacteria, fungi, and some viruses [20].
Perhaps, in conditions of persistent infection during pregnancy, the immune response is characterized by a gra–dual change in the balance of cytokines with an increase in the level of pro-inflammatory and a decrease in anti-inflammatory cytokines in all biological environments. A clinical picture of secondary immunodeficiency with the formation of a systemic inflammatory response syndrome appears in the body, including musculoskeletal system. In the case of a genetic predisposition combined with the influence of epigenetic factors, the formation of the disease is observed. As for diseases of the musculoskeletal system, VD deficiency status can be an important factor, when it comes to both the direct disturbance of calcium-phosphorus homeostasis and the immunomodulatory effect of calcitriol.
According to our results, the average level of VD in the blood of pregnant women with HIR was 1.4 times lower than that of healthy pregnant women (31.73 ± 9.00 vs. 43.38 ± 13.41 ng/ml, Uemp = 2097.5; р = 0.0009) that is, the difference between the groups is 11.7 ng/ml. According to Danese E. et al. [8], in conditions of a decrease in 25(OH)D level between groups of pregnant women with and wi–thout gestational diabetes in the amount of 4.93–7.36 nmol/l (1.97–2.94 ng/ml) and between groups with and without preeclampsia in the amount of 3.86–14.53 nmol/l (1.5–5.8 ng/ml) is already accompanied by the deterioration of perinatal consequences.
The number of pregnant women with insufficient (37.5 % (21 persons)) or deficient (39.3 % (22 subjects)) VD status among women with HIR deserves attention: the optimal VD level was found only in every 5 women (23.6 %) of the main group, and in the control group (85 % of pregnant females (F = 0.00001; p = 0.00001)). According to Saraf R. et al. [21], the prevalence of VD insufficiency or deficiency in pregnant women in America is 64 and 9 %, and in Europe — 57 and 23 %.
These results may indicate the direct involvement of calcitriol in the formation of the clinical syndrome of the inflammatory response and placental dysfunction caused by morpho-functional changes and violations of adaptive and compensatory mechanisms in the placenta. Probably, the role of calcitriol is not limited to its participation in the re–gulation of calcium homeostasis: under HIR conditions, the immunomodulatory effect of VD increases, and perhaps the low level of VD in pregnant women may be due not only to its nutritional insufficiency and impaired synthesis but also to ordinary participation in the systemic inflammatory and immunological reaction of the body. As a result of immunological imbalance, a violation of cytokine regulation of the gestational process and a complicated course of pregnancy and childbirth can be observed.
Determination of genotypes by Bsml polymorphism of the VDR gene showed that in pregnant women with HIR, the heterozygous combination of alleles — the A/G genotype is dominant (67.7 vs. 35 %; OR = 3.8; 95% CI: 2.1–6.8; χ2 = 20.88; p = 0.00001). This allows us to talk about a greater risk of developing of infectious pathology in women with this genotype in conditions of impaired VD status. On the contrary, the number of women — homozygotes with the G/G genotype was higher among healthy pregnant women (47.50 vs. 19.6 % of women; OR = 0.27; 95% CI: 0.15–0.51; χ2 = 16.7, p = 0.00006); probably, the risk of infection is lower in this group. That is, VD status in the presence of a genetic predisposition to the formation of pathology acts as an epigenetic factor on which the probability of the formation of pathology depends, in particular, we consider the risk of infection, the probability of diseases of the musculoskeletal system (joints), and the complicated course of pregnancy.
As mentioned earlier, diseases of the musculoskeletal system were present in every third pregnant woman with GI (32.14 vs. 12.5 %; OR = 3.15; 95% CI: 1.54–6.46). Among them reactive arthritis (10.7 %), osteochondrosis of the spine (most often in the lumbar spine, 10.7 %), less often fractures (3.6 %), Schmorl’s nodes (5.5 %), and osteomyelitis (1.8 %). The study of the Bsml polymorphism of VDR gene among pregnant women with diseases of the musculoskeletal system showed that most of them have the heterozygous genotype A/G (71.43 % — 13 subjects), the other 28.6 % (5 persons) are homozygotes — carriers of the A allele/A. That is, the Bsml polymorphic type of the gene encoding VDR may be important in the development of joint diseases in women with calcitriol deficiency/insufficiency, but further studies are needed due to the small number of study participants.
It should be emphasized that we operated only on anamnesis data: the pregnant women did not take any specific medications; there were no cases of disease activation and no need for additional examinations and consultations du–ring pregnancy. According to the data of Ince-Askan H. and co-authors (2017), in patients with polyarthritis and a low level of disease activity in the 1st trimester (regardless of the status of autoantibodies or taking corticosteroids), in most cases, remission of seizures is also observed in the 3rd trimester [22].
The risks of infection during pregnancy have several possible explanations. Suppression of specific and activation of non-specific immunity, changes in the hormonal profile associated with a high level of estrogens, etc. A decrease in the expression of placental histocompatibility antigen G (human leukocyte antigens — HLA-G), and an increase in the production of pro-inflammatory cytokines create conditions for the development of an inflammatory response and endothelial dysfunction. It is precise because of changes in the body’s immune system that women rarely make a primary diagnosis of rheumatic diseases during pregnancy. In addition, the physiological changes during pregnancy can often hide the clinical picture in a patient who has joint pain and weakness [12]. In the patients of the examined group, the diagnosis of rheumatoid arthritis was never detected either by anamnesis or by clinical data during the pregnancy.
Thus, data from the literature on the skeletal and pleiotropic effects of calcitriol, its participation in the realization of reproductive potential, taking into account its immunomodulatory effect and participation in the formation of the systemic inflammatory reaction syndrome, as well as the results of our own research, allow us to draw a number of conclusions.
Limitations of the study. The studied population of pregnant women with musculoskeletal system diseases was small, the diagnosis of diseases was based only on the data of the woman’s history and the results of the examination before pregnancy, which significantly limits the power of the study and therefore requires caution when interpreting the results — further targeted studies are needed.
Conclusions
In 80 % of pregnant women with HIR the VD status is characterized by deficiency or insufficiency. The HIR is caused by the presence of mixed viral-bacterial-fungal associations, including a group of TORCH infections. The peculiarities of the general somatic anamnesis in pregnant women at HIR, along with the high frequency of kidney di–seases (37.5 %), include the pathology of the musculoske–letal system diseases, which was noted in 32.1 % of pregnant woman from this group. The study of the single-nucleotide polymorphism of the Bsml gene encoding calcitriol receptors showed that among pregnant females with HIR, 67.7 % of subjects are heterozygotes with the A/G genotype, which suggests a higher probability of infection in conditions of VD insufficiency or deficiency in these persons. The study of the genetic characteristics of women with the pathology of the musculoskeletal system showed that the heterozygous A/G genotype also dominates among them, but the small sample size requires further research.
It seems appropriate to further study the status of VD and the features of the genetic coding of its receptors in women with complicated pregnancy and various extragenital pathologies, which will make it possible to personalize risks and carry out timely correction of the modifiable factors, in particular, VDD, in order to improve perinatal outcomes for women and newborns.
Received 13.10.2022
Revised 28.02.2023
Accepted 28.02.2023

/31.jpg)
/32.jpg)