
Международный эндокринологический журнал Том 19, №4, 2023
Вернуться к номеру
Роль кортизолу у формуванні метаболічного синдрому в дітей: дані літератури та власне спостереження

Авторы: N. Gromnatska, I. Pasichnyuk, O. Tomashevska
Danylo Halytsky Lviv National Medical University, Lviv, Ukraine
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
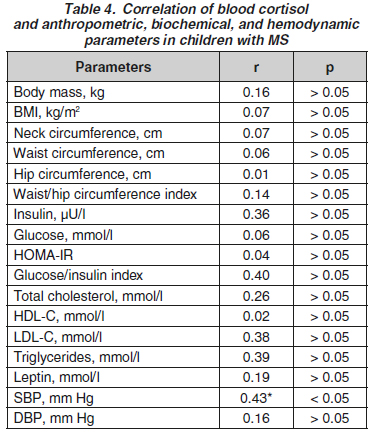
Актуальність. Розглядається питання патогенетичного впливу кортизолу на розвиток метаболічного синдрому (МС) у дітей. Надпорогові значення кортизолу пропонують вважати маркером МС. Мета: вивчити зв’язок між кортизолом і компонентами МС у дітей. Матеріали та методи. Обстежено 44 дитини з МС (група дослідження; окружність талії > 90-го перцентиля розподілу згідно з віком і статтю) та 14 дітей без ознак МС (група контролю). Діти досліджуваних груп не відрізнялись за віком та статтю. Визначали антропометричні показники (маса тіла, зріст, індекс маси тіла, окружність шиї, талії та стегон, індекс окружність талії/окружність стегон), кортизол та лептин крові, ліпідний та вуглеводний спектр крові (загальний холестерин, холестерин ліпопротеїнів високої та низької щільності, тригліцериди, глюкоза та інсулін крові, HOMA-IR, індекс глюкоза/інсулін). Проводили триразове вимірювання артеріального тиску з підрахунком середнього показника. Діагноз сформований згідно з рекомендаціями IDF, 2007. Результати. Установлено, що рівень кортизолу крові в дітей із МС (362,9 (255,5–634,1) мкг/л) на 37,9 % нижчий, ніж у контрольній групі (р > 0,05). Частота надпорогових значень кортизолу крові в дітей двох груп становила 31,8 та 50,0 % відповідно (р > 0,05). Вивчення залежності кортизолу крові від антропометричних показників (rmax = 0,16; р > 0,05), показників ліпідного (rmax = 0,4; р > 0,05) та вуглеводного обміну (rmax = 0,26; p > 0,05), лептину крові (r = 0,19; р > 0,05) з використанням коефіцієнта кореляції Спірмена вірогідності не виявило. Установлено вірогідну залежність між кортизолом і систолічним артеріальним тиском. Висновки. У пацієнтів із МС не встановлено вірогідної різниці в рівнях кортизолу крові порівняно з дітьми без критеріїв МС. Не доведено асоціацію кортизолу крові з критеріями МС, крім систолічного артеріального тиску. Кортизол не може слугувати маркером МС, хоча і має патогенетичне значення у формуванні артеріального тиску в дітей із МС, тому що гемодинамічна складова не є критерій-утворюючою ознакою.
Background. The issue of the pathogenetic influence of cortisol on the development of metabolic syndrome (MS) in children is considered. The above-threshold values of cortisol are proposed to be taken as a marker of MS. The purpose was to study the relationship between blood cortisol and MS components in children. Materials and methods. We have examined 44 children with MS (study group; waist circumference > 90th percentile of the distribution according to age and sex) and 14 children without signs of MS (controls). The children of the study groups did not differ in age and gender. Anthropometric parameters (body weight, height, body mass index, neck, waist, and hip circumferences, waist/hip circumference index), blood cortisol and leptin, blood lipid and carbohydrate spectrum (total cholesterol, high- and low-density lipoprotein cholesterol, triglycerides, blood glucose, and insulin, HOMA-IR and glucose/insulin indices) were evaluated. The measurement of blood pressure with the calculation of the average level was conducted three times. The diagnosis of MS was formed according to the IDF guidelines, 2007. Results. It was found that the level of blood cortisol in children with MS (362.9 (255.5–634.1) µg/l) was 37.9 % lower than in controls (р > 0.05). The frequency of the above-threshold blood cortisol values in children of both groups was 31.8 and 50.0 %, respectively (р > 0.05). The study of dependence using the Spearman’s rank correlation coefficient between blood cortisol and anthropometric parameters (rmax = 0.16; p > 0.05), lipids (rmax = 0.4; р > 0.05), carbohydrate metabolism (rmax = 0.26; р > 0.05), and blood leptin (r = 0.19; р > 0.05) did not reveal any significance. A significant correlation was found between cortisol and systolic blood pressure. Conclusions. In children with MS, there was no significant difference in the level of blood cortisol compared to those without MS criteria. The association of blood cortisol and MS criteria other than systolic blood pressure has not been found. Although cortisol is important in the formation of systolic blood pressure, it cannot serve as a marker of MS in children since it is not a criterion-forming sign of MS.
метаболічний синдром; кортизол; діти
metabolic syndrome; cortisol; children
Introduction
Materials and methods
Results

Discussion
Conclusions
- Zimmet P., Alberti K.G., Kaufman F., Tajima N., Silink M. et al.; IDF Consensus Group. The metabolic syndrome in children and adolescents — an IDF consensus report. Pediatr. Diabetes. 2007 Oct. 8(5). 299-306. doi: 10.1111/j.1399-5448.2007.00271.x.
- Weihe P., Weihrauch-Blüher S. Metabolic syndrome in children and adolescents: diagnostic criteria, therapeutic options, and perspectives. Curr. Obes. Rep. 2019 Dec. 8(4). 472-479. doi: 10.1007/s13679-019-00357-x.
- Morton N.M., Seckl J.R. 11beta-hydroxysteroid dehydrogenase type 1 and obesity. Front. Horm. Res. 2008. 36. 146-164. doi: 10.1159/000115363.
- Vogelzangs N., Beekman A.T., Dik M.G., Bremmer M.A., Comijs H.C. et al. Late-life depression, cortisol, and metabolic syndrome. Am. J. Geriatr. Psychiatry. 2009 Aug. 17(8). 716-21. doi: 10.1097/JGP.0b013e3181aad5d7.
- Garcez A., Leite H.M., Weiderpass E., Paniz V.M.V., Watte G. et al. Basal cortisol levels and metabolic syndrome: a systematic review and meta-analysis of observational studies. Psychoneuroendocrinology. 2018 Sep. 95. 50-62. doi: 10.1016/j.psyneuen.2018.05.023. doi: 10.1016/j.psyneuen.2018.05.023.
- Reinehr T., Kulle A., Wolters B., Knop C., Lass N. et al. Relationships between 24-hour urinary free cortisol concentrations and metabolic syndrome in obese children. J. Clin. Endocrinol. Metab. 2014 Jul. 99(7). 2391-9. doi: 10.1210/jc.2013-4398.
- DuBose K.D., McKune A.J. The relation between salivary cortisol and the metabolic syndrome score in girls. J. Pediatr. Endocrinol. Metab. 2013. 26(9–10). 841-7. doi: 10.1515/jpem-2012-0415.
- Mazgelytė E., Mažeikienė A., Burokienė N., Matuzevičienė R., Linkevičiūtė A. et al. Association between hair cortisol concentration and metabolic syndrome. Open Med. (Warsaw). 2021 Jun 16. 16(1). 873-881. doi: 10.1515/med-2021-0298.
- Van der Valk E.S., Savas M., van Rossum E.F.C. Stress and Obesity: Are There More Susceptible Individuals? Curr. Obes. Rep. 2018 Jun. 7(2). 193-203. doi: 10.1007/s13679-018-0306-y.
- Kjölhede E.A., Gustafsson P.E., Gustafsson P.A., Nelson N. Overweight and obese children have lower cortisol levels than normal-weight children. Acta Paediatr. 2014 Mar. 103(3). 295-9. doi: 10.1111/apa.12499.
- Sen Y., Aygun D., Yilmaz E., Ayar A. Children and adolescents with obesity and metabolic syndrome have high circulating cortisol levels. Neuroendocrinol. Lett. 2008 Feb. 29(1). 141-5.
- Özçelik E., Uslu S., Kebapçı N., Kara M., Dokumacıoğlu A., Musmul A. Interrelations of serum leptin levels with adrenocorticotropic hormone, basal cortisol, and dehydroepiandrosterone sulfate levels in patients with metabolic syndrome. Diabetes and Metabolic Syndrome: Clinical Research and Reviews. 2010. 4(1). 13-17. doi: 10.1016/j.dsx.2010.01.005.
- Michels N., Sioen I., Schraven K., De Decker A., van Aart C., De Henauw S. Children’s cortisol and externalizing stress symptoms are predictors of adiponectin evolution over two years. Biol. Psychol. 2018 Jan. 131. 89-95. doi: 10.1016/j.biopsycho.2017.05.016.
- Anagnostis P., Athyros V.G., Tziomalos K., Karagiannis A., Mikhailidis D.P. Clinical review: the pathogenetic role of cortisol in the metabolic syndrome: a hypothesis. J. Clin. Endocrinol. Metab. 2009 Aug. 94(8). 2692-701. doi: 10.1210/jc.2009-0370.
- Jin S., Sun X., Liu Q., Liang H., Li C., Mao Z. et al. Steroid hormones in cord blood mediate the association between maternal prepregnancy BMI and birth weight. Obesity. 2019. 27. 1338-46.
- Ricotti R., Solito A., Mariotti Zani E., Caputo M., Genoni G. et al. The relationship between cortisol and IGF-I influences metabolic alteration in pediatric overweight and obesity. Eur. J. Endocrinol. 2020 Mar. 182(3). 255-264. doi: 10.1530/EJE-19-0792.
- Krishnaveni G.V., Veena S.R., Dhube A., Karat S.C., Phillips D.I., Fall C.H. Size at birth, morning cortisol and cardiometabolic risk markers in healthy Indian children. Clin. Endocrinol. (Oxford). 2014 Jan. 80(1). 73-9. doi: 10.1111/cen.12143.
- Kraemer W.J., Ratamess N.A., Hymer W.C., Nindl B.C., Fragala M.S. Growth Hormone(s), Testosterone, Insulin-Like Growth Factors, and Cortisol: Roles and Integration for Cellular Development and Growth With Exercise. Front. Endocrinol. (Lausanne). 2020 Feb 25. 11. 33. doi: 10.3389/fendo.2020.00033.
- Hewagalamulage S.D., Lee T.K., Clarke I.J., Henry B.A. Stress, cortisol, and obesity: a role for cortisol responsiveness in identifying individuals prone to obesity. Domest. Anim. Endocrinol. 2016 Jul. 56 Suppl. S112-20. doi: 10.1016/j.domaniend.2016.03.004.
- Gromnatska N., Lemishko B., Kulya O., Pasichna I., Beliusova V. Screening of metabolic syndrome in children and adolescents. International Journal of Endocrinology (Ukraine). 2022. 18(2). 94-99. doi: 10.22141/2224-0721.18.2.2022.1153.
- Martens A., Duran B., Vanbesien J., Verheyden S., Rutteman B. et al. Clinical and biological correlates of morning serum cortisol in children and adolescents with overweight and obesity. PLoS One. 2021 Oct 20. 16(10). e0258653. doi: 10.1371/journal.pone.0258653.
- Weigensberg M.J., Toledo-Corral C.M., Goran M.I. Association between the metabolic syndrome and serum cortisol in overweight Latino youth. J. Clin. Endocrinol. Metab. 2008 Apr. 93(4). 1372-8. doi: 10.1210/jc.2007-2309.
- Abraham S.B., Rubino D., Sinaii N., Ramsey S., Nieman L.K. Cortisol, obesity, and the metabolic syndrome: a cross-sectional study of obese subjects and review of the literature. Obesity (Silver Spring). 2013 Jan. 21(1). E105-17. doi: 10.1002/oby.20083.