
Журнал «Медицина неотложных состояний» Том 22, №2, 2026
Вернуться к номеру
Ефективність ESP-блоку для знеболювання резекції легень: проспективне рандомізоване контрольоване дослідження
Авторы: A.P. Perkonos, I.I. Lisnyy
Natonal Cancer Institute, Kyiv, Ukraine
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
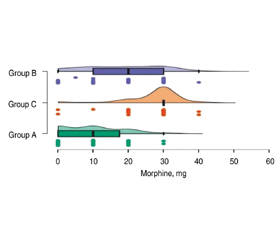
Актуальність. Резекції легень, виконані за допомогою торакотомного доступу, супроводжуються значною хірургічною травмою. Забезпечення адекватного знеболювання таких втручань є складним викликом для анестезіолога. Для періопераційного знеболювання в торакальній хірургії доречно використовувати регіонарні методи. ESP-блок є відносно новим регіонарним методом знеболювання, ефективність якого потребує вивчення, зокрема в торакальній хірургії. Мета: визначити ефективність ESP-блоку для знеболювання резекції легень із класичним торакотомним доступом порівняно з іншими, традиційними методами, а саме знеболюванням із застосуванням торакальної епідуральної анестезії (ТЕА), а також без використання регіонарних технік. Матеріали та методи. Проведено оцінку якості знеболювання у 131 пацієнта, яким виконували резекцію легень. Учасників випадковим способом розподілили на 3 групи: групу A (ТЕА), групу B (ESP-блок) та групу C (без регіонарного знеболювання, контрольна група). Визначали інтенсивність больового синдрому за візуальною аналоговою шкалою в спокої та при глибокому вдиху; якість сну за 5-бальною шкалою протягом трьох післяопераційних діб; рівень маркерів стрес-реакції (глюкоза, кортизол) інтраопераційно та післяопераційно; кількість використаного морфіну післяопераційно. Результати. Інтенсивність больового синдрому була нижчою в групах A та B порівняно з групою C; показники стрес-реакції статистично не відрізнялись між групами; якість сну була кращою в групі А на 3-тю добу; потреба в морфіні в післяопераційний період була меншою в групі ТЕА та ESP-блоку, ніж у контрольній групі. Висновки. ESP-блок може бути рекомендований як компонент періопераційного знеболювання торакальних операцій та розглядатися як альтернативний метод регіонарного знеболювання у випадках, коли ТЕА протипоказана.
Background. Lung resection procedures performed via a conventional thoracotomy are associated with substantial surgical trauma and pronounced postoperative pain. Providing adequate perioperative analgesia for such interventions remains a significant challenge for anesthesiologists. In thoracic surgery, the use of regional analgesia techniques is considered appropriate. The erector spinae plane (ESP) block is a relatively novel regional analgesia technique, the effectiveness of which — particularly in thoracic surgery — requires further investigation. The purpose is to evaluate the effectiveness of the ESP block for analgesia in lung resection surgery performed via a conventional thoracotomy, in comparison with thoracic epidural analgesia (TEA) and analgesia without regional techniques. Materials and methods. A prospective randomized controlled study was conducted involving 131 patients undergoing lung resection. They were randomly assigned to three groups: group A — TEA, group B — ESP block, and group C — no regional analgesia (controls). Pain intensity was assessed using the visual analog scale at rest and during deep inspiration; sleep quality was evaluated using a five-point scale over the first three postoperative days. Markers of stress response (glucose and cortisol) were measured intraoperatively and postoperatively, and cumulative postoperative morphine consumption was recorded. Results. Postoperative pain intensity was significantly lower in the TEA and ESP block groups compared to the control one. Levels of stress-response markers did not differ significantly between groups. Sleep quality was superior in the TEA group on the third postoperative day. Postoperative morphine requirements were lower in the TEA and ESP block groups than in the group without regional analgesia. Conclusions. The ESP block is an effective component of perioperative analgesia for thoracic surgery and may be considered an alternative regional analgesia technique in patients with contraindications to thoracic epidural analgesia.
ESP-блок; торакальна епідуральна анестезія; резекція легень; торакотомія; післяопераційний біль; регіонарне знеболювання; мультимодальна аналгезія
erector spinae plane block; thoracic epidural analgesia; lung resection; thoracotomy; postoperative pain; regional analgesia; multimodal analgesia
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Mesbah A, Yeung J, Gao F. Pain after thoracotomy. BJA Educ. 2016 Jan;16(1):1-7. doi: 10.1093/bjaceaccp/mkv005.
- Pennefather SH, McKevith J. Pain management after thoracic surgery. In: Slinger P, ed. Principles and practice of anesthesia for thoracic surgery. New York: Springer; 2011. 675-699. doi: 10.1007/978-1-4419-0184-2_46.
- Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, Brunelli A, Cerfolio RJ, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. 2019 Jan 1;55(1):91-115. doi: 10.1093/ejcts/ezy301.
- Sarridou DG, Mouratoglou SA, Mitchell JB, Cox F, Boutou A, et al. Post-Operative Thoracic Epidural Analgesia and Incidence of Major Complications according to Specific Safety Standardized Documentation: A Large Retrospective Dual Center Experience. J Pers Med. 2023 Nov 29;13(12):1672. doi: 10.3390/jpm13121672.
- Feray S, Lubach J, Joshi GP, Bonnet F, Van de Velde M; PROSPECT Working Group of the European Society of Regional –Anaesthesia and Pain Therapy. PROSPECT guidelines for video-assisted thoracoscopic surgery: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2022 Mar;77(3):311-325. doi: 10.1111/anae.15609.
- Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The Erector Spinae Plane Block: A Novel Analgesia technique in Thoracic Neuropathic Pain. Reg Anesth Pain Med. 2016 Sep-Oct;41(5):621-7. doi: 10.1097/AAP.0000000000000451
- Greisen J, Juhl CB, Grøfte T, Vilstrup H, Jensen TS, Schmitz O. Acute pain induces insulin resistance in humans. Anesthesiology. 2001 Sep;95(3):578-84. doi: 10.1097/00000542-200109000-00007.
- Cusack B, Buggy DJ. Anaesthesia, analgesia, and the surgical stress response. BJA Educ. 2020 Sep;20(9):321-328. doi: 10.1016/j.bjae.2020.04.006.
- Lehrke M, Broedl UC, Biller-Friedmann IM, Vogeser M, Henschel V, et al. Serum concentrations of cortisol, interleukin 6, leptin and adiponectin predict stress induced insulin resistance in acute inflammatory reactions. Crit Care. 2008;12(6):R157. doi: 10.1186/cc7152.
- Chou R, Gordon DB, de Leon-Casasola OA, Rosenberg JM, Bickler S, et al. Management of Postoperative Pain: A Clinical Practice Guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016 Feb;17(2):131-57.
- Pöpping DM, Elia N, Marret E, Remy C, Tramèr MR. Protective effects of epidural analgesia on pulmonary complications after abdominal and thoracic surgery: a meta-analysis. Arch Surg. 2008 Oct;143(10):990-9; discussion 1000. doi: 10.1001/archsurg.143.10.990.
- ESRA-Europe. Summary recommendations: thoracotomy. PROSPECT Working Group; 2015. Available from: https://esraeurope.org/wp-content/uploads/2019/02/Summary-recommendations_Thoracotomy_ENG.pdf.
- NYSORA. Epidural anesthesia & analgesia. Albany (NY): NYSORA. Available from: https://www.nysora.com/topics/abdomen/epidural-anesthesia-analgesia/#toc_PHYSIOLOGICEFFECTSOFEPIDURALblock.
- Lisnyy II, Semenyshyna KG, Vlasiuk HR, Balaban TP, Zakalska KhA, et al. Infection rate and bacterial flora of the epidural catheter during prolonged epidural analgesia in patients after oncological surgery. Emergency Medicine (Ukraine). 2025;21(5):459-470. doi: 10.22141/2224-0586.21.5.2025.1911.