
Журнал «Травма» Том 27, №2, 2026
Вернуться к номеру
Малоінвазивна гібридна фіксація та реабілітація при переломах надп’ятково-гомілкового суглоба типу B/C за Danis-Weber у пацієнтів із цукровим діабетом: порівняльні результати
Авторы: U.V. Kuz (1), Yu.O. Divnych (2), I.M. Gudz (1), S.M. Vasyliuk (1), Ye.V. Nychvyd (1), V.I. Dubas (1), V.P. Omelchuk (1), V.S. Sulyma (1)
(1) - Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine
(2) - University of Bern, Bern, Switzerland
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
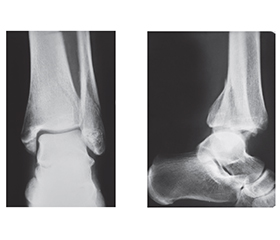
Актуальність. Хірургічне лікування пацієнтів із діабетом та переломом надп’ятково-гомілкового суглоба (НГС) є складним через високий ризик ускладнень, як-от стопа Шарко. Мета: покращити ефективність хірургічного лікування та реабілітації хворих на діабет із переломами НГС. Матеріали та методи. Дослідження провели у 31 пацієнта з переломами НГС типу B і С за класифікацією Danis-Weber. У 7 осіб із діабетом І (дослідної) групи виконано малоінвазивний (гібридний) остеосинтез за оригінальною методикою (патент № 134463); у 9 пацієнтів ІІ (порівняльної) групи без діабету, але з вираженими післятравматичними ознаками ушкодження м’яких тканин провели аналогічний остеосинтез; у 15 осіб ІІІ (контрольної) групи без хронічних патологій — остеосинтез пластиною з фіксацією дистального міжгомілкового синдесмозу позиційним шурупом. Ризик післяопераційних ускладнень у І групі прогнозували за шкалою Adelaide Fracture in the Diabetic Ankle (AFDA). Якість хірургічного лікування оцінювали за відновленням рентгеноморфометричних параметрів. Ефективність реабілітації визначали за опитувальниками American Orthopaedic Foot and Ankle Score (AOFAS) та Olerud-Molander Ankle Score (OMAS) на 4-й і 8-й тиждень після операції та через 6 місяців. Результати. Згідно з післяопераційними рентгенологічними даними, в усіх групах досягнуто відновлення анатомічних структур НГС (p < 0,05). Суттєвих відмінностей у наявності ознаки dime/ball між групами не виявлено ( = 0,2609; p = 0,26). Щодо функціональних результатів за шкалою AOFAS у післягострому періоді (4–8 тижнів), у пацієнтів І та ІІ груп (гібридний остеосинтез) спостерігали позитивну динаміку відновлення функції суглоба (p < 0,05), а у віддаленому періоді реабілітації (6 місяців) показники між групами статистично не відрізнялися (p = 0,1158). Натомість, за опитувальником OMAS, після гібридного остеосинтезу пацієнти мали кращі функціональні результати в післягострому періоді (4-й тиждень). На 8-му тижні в усіх групах досягнуто однаковий рівень відновлення, а на 6-му місяці у ІІ та ІІІ групах виявили вірогідно кращі результати, ніж у контрольній (р = 0,02354). Висновки. В осіб із діабетом та переломами НГС Danis-Weber типу B і С, які мають високий ризик післяопераційних ускладнень за шкалою AFDA, слід виконувати інтрамедулярний гібридний остеосинтез, що мінімізує ушкодження м’яких тканини при операції, та застосовувати індивідуальний протокол реабілітації, що надалі може запобігти виникненню стопи Шарко.
Background. Surgical treatment of ankle fractures in diabetic patients is challenging due to the high risk of complications such as Charcot foot. The purpose was to enhance the effectiveness of surgical treatment and rehabilitation for ankle fractures in patients with diabetes. Materials and methods. Research was conducted on 31 patients with Danis-Weber type B and C ankle fractures: group I (study) — 7 diabetic patients treated with minimally invasive osteosynthesis using an original technique (patent No. 134463); group II (comparative) — 9 non-diabetic patients with post-traumatic signs of soft tissue damage undergone similar osteosynthesis; group III (control) — 15 patients without chronic disease, treated with fibular plate osteosynthesis and syndesmosis fixation using a positional screw. In group I, complication risk was assessed using the Adelaide Fracture in the Diabetic Ankle (AFDA) scale. Surgical treatment quality was evaluated with X-ray morphometric parameters restoration. Rehabilitation effectiveness was measured by the American Orthopaedic Foot and Ankle Society (AOFAS) scale and Olerud-Molander Ankle Score (OMAS) at 4 and 8 weeks and 6 months after surgery. Results. Post-operative X-ray data confirm restoration of ankle anatomy in all groups (p < 0.05). No significant differences in dime/ball sign presence were observed between groups ( = 0.2609; p = 0.26). Functional assessment using the AOFAS scale showed no statistically significant difference among the groups (p = 0.1158). In terms of functional outcomes in the post-acute period (4–8 weeks) according to the AOFAS, patients of groups I and II (hybrid osteosynthesis) had positive dynamics of the joint recovery process (p < 0.05), and in the long-term rehabilitation period (6 months), the indicators did not differ between the groups (p = 0.1158). In contrast, according to the OMAS, after hybrid osteosynthesis, functional outcomes were better in the post-acute period (4 weeks). At 8 weeks, patients of all groups achieved the same level of recovery, and at 6 months, significantly better results were observed in groups II and III than in controls (p = 0.02354). Conclusions. Patients with diabetes and Danis-Weber type B or C ankle fractures who have a high AFDA-assessed risk of postoperative complications should undergo intramedullary hybrid osteosynthesis, which minimizes secondary soft-tissue damage during surgery, and follow an individualized rehabilitation protocol to further prevent the development of Charcot foot.
перелом надп’ятково-гомілкового суглоба; цукровий діабет; малоінвазивні хірургічні втручання; реабілітація
ankle fracture; diabetes mellitus; minimally invasive surgical procedures; rehabilitation