
Журнал «Травма» Том 27, №2, 2026
Вернуться к номеру
Клініко-епідеміологічна характеристика посттравматичної нейропатії сідничного нерва в постраждалих із пошкодженням кульшової западини
Авторы: S.O. Guryev (1), M.L. Ankin (2), M.M. Barylovych (2), H.P. Kushnir (3)
(1) - Ukrainian Scientific and Practical Center of Emergency Medical Care and Disaster Medicine of MHU,
Kyiv, Ukraine
(2) - Shupyk National Healthcare University of Ukraine, Kyiv, Ukraine
(3) - Central Polyclinic of the MIA of Ukraine, Kyiv, Ukraine
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
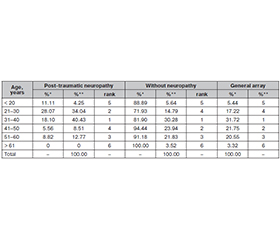
Актуальність. Пошкодження кульшової западини, за даними джерел наукової інформації, виникає внаслідок високоенергетичної травми. До 33 % таких випадків може супроводжуватися розвитком посттравматичної нейропатії сідничного нерва. Мета: вивчити клініко-епідеміологічні характеристики посттравматичної нейропатії сідничного нерва в постраждалих із переломом кульшової западини. Матеріали та методи. Проведено ретроспективний аналіз 331 випадку пошкодження кульшової западини. Загальний масив розподілено на дві групи: 284 пацієнти з пошкодженням кульшової западини без посттравматичної нейропатії та 47 — із посттравматичною нейропатією сідничного нерва. Дослідження проведено із застосуванням параметричних і непараметричних методів статистики, а також елементів фрактального аналізу. Результати. Встановлено, що всі клініко-епідеміологічні ознаки є факторами ризику посттравматичної нейропатії в постраждалих із переломом кульшової западини. Серед осіб із нейропатією переважають чоловіки (74,47 %), але ризик полінейропатії є вищим у жінок. Посттравматична нейропатія при переломі кульшової западини в основному зустрічається в постраждалих найбільш активного, працездатного віку 21–40 років (74,47 %). Найчастіше посттравматична нейропатія виникає при отримані пошкодження під час прямого удару — 91,50 %. Основними обставинами травми є дорожньо-транспортні пригоди (91,48 %), за яких найчастіше розвивається посттравматична нейропатія в постраждалих із переломом кульшової западини, а найрідше — при побутовій травмі (2,13 %). Висновки. 1. Встановлено, що клініко-епідеміологічні ознаки пацієнтів із переломами кульшової западини мають вірогідний вплив на виникнення посттравматичної нейропатії сідничного нерва. 2. Найчастіше вона трапляється внаслідок перелому кульшової западини у жінок (19,35 % цієї статевої групи), осiб віком 21–30 років (28,07 % цієї вікової групи), внаслідок прямого удару (28,10 % групи «механізм пошкодження») та при дорожньо-транспортних пригодах (20,38 % групи «обставини травми»). 3. Усі клініко-епідеміологічні ознаки є факторами ризику нейропатії сідничного нерва в постраждалих із переломами кульшової западини. 4. Потрібні подальші ризик-орієнтовані дослідження клініко-епідеміологічних аспектів виникнення посттравматичної нейропатії сідничного нерва як ускладнення переломів кульшової западини.
Background. According to the scientific sources, hip socket damage in victims occurs as a result of high-energy trauma. Up to 33 % of such cases may be accompanied by the development of post-traumatic sciatic nerve neuropathy. The purpose was to study and form the clinical and epidemiological characteristics of post-traumatic sciatic nerve neuropathy in victims with hip fracture. Materials and methods. A retrospective analysis of 331 cases of hip socket injury was conducted. The total array was divided into two groups: 284 patients with hip socket injury without post-traumatic neuropathy, and 47 cases with post-traumatic sciatic nerve neuropathy. The study was conducted using parametric and non-parametric statistical methods, as well as elements of fractal analysis. Results. It was found that all clinical and epidemiological signs are a risk factor for the occurrence of post-traumatic neuropathy in hip fractures. Among victims with neuropathy, men predominate (74.47 %), but the risk of polyneuropathy is higher in women. Post-traumatic neuropathy in hip fractures mainly occurs in people of the most active, able-bodied age of 21–40 years (74.47 %). Most often, post-traumatic neuropathy is a result of a direct impact — 91.50 %. The main circumstance of injury are road accidents (91.48 %), in which post-traumatic neuropathy most often develops in victims with hip fracture, and most rarely — with household trauma (2.13 %). Conclusions. 1. It has been found that the clinical and epidemiological characteristics of patients with hip fractures have a probable influence on the occurrence of post-traumatic sciatic nerve neuropathy. 2. Most often, post-traumatic sciatic nerve neuropathy occurs as a result of hip fracture in women (19.35 % of this gender group), people aged 21–30 years (28.07 % of this age group), as a result of direct impact (28.10 % of this group by mechanism of injury) and in traffic accidents — 20.38 % (group of circumstances of injury). 3. All clinical and epidemiological signs are risk factors for the occurrence of sciatic nerve neuropathy in hip fractures. 4. Further risk-based studies of the clinical and epidemiological aspects of the occurrence of post-traumatic sciatic neuropathy as a complication of hip fractures are needed.
нейропатія; сідничний нерв; кульшова западина; перелом; постраждалі
neuropathy; sciatic nerve; hip socket; fracture; injured