
Архив офтальмологии Украины Том 14, №1, 2026
Вернуться к номеру
Особливості розвитку макулярного набряку після хірургічного лікування катаракти пацієнтів з цукровим діабетом 2-го типу: 1 рік спостереження
Авторы: Горохівська О.Т.
Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
Рубрики: Офтальмология
Разделы: Клинические исследования
Версия для печати
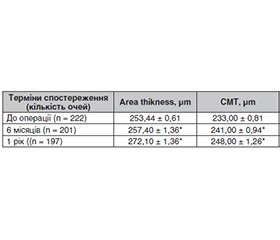
Актуальність. Діабетична ретинопатія на фоні цукрового діабету визнана основною причиною втрати зору серед населення працездатного віку як у розвинених, так і в країнах, що розвиваються. Крім того, цукровий діабет сприяє частішому виникненню та більш ранньому розвитку вікової або діабетичної катаракти. Хоча факоемульсифікація катаракти є ефективним методом лікування, зір може погіршитися після операції через прогресування або рецидив діабетичного макулярного набряку (ДМН), появу псевдофакічного макулярного набряку (ПФМН) та їх поєднання. Мета: вивчити особливості розвитку макулярного набряку після хірургічного лікування катаракти у пацієнтів з цукровим діабетом 2-го типу через 1 рік після втручання. Матеріали та методи. У дослідження були включені 178 пацієнтів (222 ока) віком від 45 до 76 років, із діагнозом ЦД 2-го типу, з непроліферативною діабетичною ретинопатією легкої та помірної стадії. Із них через 6 місяців після операції було обстежено 152 пацієнти (201 око) та через 1 рік — 147 пацієнтів (197 очей). Усім пацієнтам була виконана факоемульсифікація катаракти з імплантацією інтраокулярної лінзи. У післяопераційному періоді у всіх пацієнтів за даними офтальмоскопії та методу оптичної когерентної томографії було проведено дослідження розвитку ДМН, ПФМН та їх поєднання у віддалені терміни спостереження — 1 рік. Результати. У віддаленому післяопераційному періоді відзначалося вірогідне збільшення показників: area thickness через 6 місяців зросла на 1,5 %, через 1 рік — на 7,3 % від доопераційного рівня (p ≤ 0,05), центральна макулярна товщина збільшилася на 3,4 % через 6 місяців і на 6,4 % через 1 рік (p ≤ 0,05), макулярний об’єм вірогідно підвищився на 2,5 % через 6 місяців і на 4,3 % через 1 рік (p ≤ 0,05), показник співвідношення центральної товщини сітківки та об’єму сітківки також зростав поступово: +1,0 % через 6 місяців і +2,1 % через 1 рік (p ≤ 0,05). На першу добу при офтальмоскопії очного дна та за даними ОКТ не було виявлено набряків макулярної ділянки. Офтальмоскопічно та за даними ОКТ через 6 місяців ДМН було діагностовано в 14,9 % випадків; поєднання ДМН та ПФМН — у 4,47 % випадків. Через 1 рік ДМН, ПФМН було діагностовано в 9,13 та 5,44 % випадків відповідно. Через 1 рік відмічалось поєднання ДМН та ПФМН в 1,01 % випадків. Висновки. Встановлено, що ПФМН або поєднання ДМН і ПФМН є не частим, але типовим ускладненням сучасної технології хірургічного лікування катаракти у пацієнтів з цукровим діабетом 2-го типу й легкою та помірною непроліферативною діабетичною ретинопатією.
Background. Diabetic retinopathy associated with diabetes mellitus is recognized as the leading cause of vision loss among the working-age population in both developed and developing countries. In addition, diabetes mellitus contributes to a higher incidence and earlier onset of age-related or diabetic cataract. Although phacoemulsification is an effective treatment, vision may deteriorate after surgery due to the progression or recurrence of diabetic macular edema (DME), the development of pseudophakic cystoid macular edema (PCME), or a combination of both. The purpose: to study the features of the macular edema development after cataract surgery in patients with type 2 diabetes mellitus one year after the intervention. Materials and methods. The study included 178 patients (222 eyes) aged 45 to 76 years, diagnosed with type 2 diabetes, and presenting with mild to moderate nonproliferative diabetic retinopathy. Of these, 152 patients (201 eyes) were examined 6 months after surgery, and 147 participants (197 eyes) were examined one year later. All patients underwent phacoemulsification with intraocular lens implantation. In the postoperative period, all participants underwent examination for the development of DMN, PCME, and their combination at the long-term follow-up of 1 year, based on ophthalmoscopy and optical coherence tomography (OCT). Results. In the long-term postoperative period, a statistically significant increase in the following parameters was observed: area thickness increased by 1.5 % at 6 months and by 7.3 % at 1 year compared to preoperative levels (p ≤ 0.05); central macular thickness increased by 3.4 % at 6 months and by 6.4 % at 1 year (p ≤ 0.05), macular volume significantly increased by 2.5 % at 6 months and by 4.3 % at 1 year (p ≤ 0.05), and the thickness volume ratio also increased gradually: +1.0 % at 6 months and +2.1 % at 1 year (p ≤ 0.05). On the first day, fundus ophthalmoscopy and OCT revealed no macular edema. Based on ophthalmoscopy and OCT data, DME was diagnosed in 14.9 % of cases after 6 months, a combination of DME and PCME was observed in 4.47 % of cases. One year later, DME and PCME were diagnosed in 9.13 and 5.44 % of cases, respectively, a combination of DME and PCME was observed in 1.01 % of cases. Conclusions. It has been found that PCME or a combination of DME and PCME is uncommon, but typical complication of modern surgical techniques for cataract treatment in patients with type 2 diabetes and mild to moderate nonproliferative diabetic retinopathy.
факоемульсифікація катаракти; діабетичний макулярний набряк; псевдофакічний макулярний набряк; оптична когерентна томографія
phacoemulsification; diabetic macular edema; pseu
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- World Health Organization. Diabetes. 2024 [cited 2025 May 13]. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes.
- IDF Diabetes Atlas, 10th ed. Belgium: International Diabetes Federation, 2021. Available online at: https://www.diabetesatlas.org/en.
- American Diabetes Association: Standards of Medical Care in Diabetes. Diabetes Care. 2023;46(Suppl 1):1-291.
- Serdiuk AV, Mogilevskyy SYu. Risk of ineffective treatment for diabetic retinopathy of different stages and prognostic factors that determine it. Archive of Ophthalmology of Ukraine. 2024;12(3):156-162. doi: 10.22141/2309-8147.12.3.2024.388.
- Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the international diabetes federation diabetes atlas, 9(th) edition. Diabetes Res Clin Pract. 2019;157:107843. doi: 10.1016/j.diabres.2019.107843.
- Veselovskaya ZF, Panchenko IuO, Zhupan BB, Kovtun MI, Gulida AO. Systemic risk factors for progression of diabetic retinopathy in type 2 diabetes mellitus. Archive of Ophthalmology of Ukraine. 2025;13(1):1-5. doi: 10.22141/2309-8147.13.1.2025.398.
- Натрус Л.В., Могілевський С.Ю., Панова Т.І., Риков С.О., Биховець М.Ю. Нова концепція відмінностей патогенетичних механізмів прогресування діабетичної ретинопатії у пацієнтів з цукровим діабетом 2 типу і з різним PPARγ генотипом. Офтальмологічний журнал. 2020;5:36-42. http://doi.org/10.31288/oftalmolzh202053642.
- Almutairi NM, Alahmadi S, Alharbi M, Gotah S, Alharbi M. The association between HbA1c and other biomarkers with the prevalence and severity of diabetic retinopathy. Cureus. 2021;13(1):e12520. doi: 10.7759/cureus.12520.
- Singer ME, Dorrance KA, Oxenreiter MM, Yan KR, Close KL. The Type 2 Diabetes “modern Preventable Pandemic” and Replicable Lessons from the COVID-19 Crisis. Prev. Med. Rep. 2022;25:101636.
- Parker ED, Lin J, Mahoney T, Ume N, Yang G, Gabbay RA, et al. Economic Costs of Diabetes in the U.S. in 2022. Diabetes Care. 2024;47:26-43.
- Mrugacz M, Pony-Uram M, Bryl A, Zorena K. Current Approach to the Pathogenesis of Diabetic Cataracts. IJMS. 2023;24:6317.
- Teo ZL, Tham YC, Yu M, Chee ML, Rim TH, Cheung N, et al. Global prevalence of diabetic retinopathy and projection of burden through 2045: Systematic review and meta-analysis. Ophthalmology. 2021;128(11):1580-91. doi: 10.1016/j.ophtha.2021.04.027.
- Hendrick A. Diabetes epidemic, epidemiology, statistics and trends. In: McFarlane SI, Lazzaro DR, editors. Diabetes and the eye: Latest concepts and practices. diabetes, current and future developments, vol. 2. Singapore: Bentham Science Publishers, 2021. Р. 1-12.
- Panozzo G, Staurenghi G, Dalla Mura G, Giannarelli D, Alessio G, Alongi S, et al. Prevalence of diabetes and diabetic macular edema in patients undergoing senile cataract surgery in Italy: The DIabetes and CATaract study. Eur J Ophthalmol. 2020;30(2):315-20. doi: 10.1177/1120672119830578.
- Rossi T, Panozzo G, Della Mura G, Giannarelli D, Ferrari D, Alessio G, et al. Diabetes and diabetic retinopathy in patients undergoing cataract surgery: A prevalence study-DiCat study report 2. Acta Diabetol. 2020;57(6):645-50. doi: 10.1007/s00592-019-01466-8.
- Im JHB, Jin YP, Chow R, Yan P. Prevalence of diabetic ma–cular edema based on optical coherence tomography in people with diabetes: A systematic review and meta-analysis. Surv Ophthalmol. 2022;67(4):1244-51. doi: 10.1016/j.survophthal.2022.01.009.
- Alabdulwahhab KM. Senile cataract in patients with diabetes with and without diabetic retinopathy: A community-based comparative study. J Epidemiol Glob Health. 2022;12(1):56-63. doi: 10.1007/s44197-021-00020-6.
- Alnagdy AA, Abouelkheir HY, El-Khouly SE, Tarshouby SM. Impact of topical nonsteroidal anti-inflammatory drugs in prevention of macular edema following cataract surgery in diabetic patients. Int J Ophthalmol. 2018 Apr 18;11(4):616-622. doi: 10.18240/ijo.2018.04.13.
- Chan LKY, Lin SS, Chan F, Ng DS. Optimizing treatment for diabetic macular edema during cataract surgery. Front Endocrinol (Lausanne). 2023 Jan 25;14:1106706. doi: 10.3389/fendo.2023.1106706. PMID: 36761187; PMCID: PMC9905225.
- Zarei-Ghanavati S, Hadi Y, Habibi A, Ashraf Khorasani M, Yoo SH. Cataract and diabetes: review of the literature. J Cataract Refract Surg. 2024 Dec 1;50(12):1275-1283. doi: 10.1097/j.jcrs.0000000000001547. PMID: 39254426; PMCID: PMC11556822.
- Gettinger K, Lee D, Tomita Y, Negishi K, Kurihara T. Diabetic Retinopathy, a Comprehensive Overview on Pathophysiology and Relevant Experimental Models. International Journal of Molecular Sciences. 2025;26(20):9882. https://doi.org/10.3390/ijms26209882.
- Bunjo LJ, Bacchi S, Pietris J, Weng Onn Chan. Current ma–nagement options for the treatment of refractory postoperative cystoid macular edema: A systematic review. Survey of Ophthalmology. 2024;69(Iss 4):606-621. https://doi.org/10.1016/j.survophthal.2024.03.005.
- Ivanescu A, Popescu S, Gaita L, Albai O, Braha A, Timar R. Risk Factors for Cataracts in Patients with Diabetes Mellitus. J. Clin. Med. 2024;13:7005. https://doi.org/10.3390/jcm13237005\.
- Horokhivska O. Macular edema after cataract phacoemulsification in diabetic retinopathy and type 2 diabetes mellitus. Med Sci Ukr. 2026;22(1):48-55. doi: https://doi.org/10.32345/2664-4738.1.2026.06.
- Kim M, Park YG, Park YH. Cataract surgery and the risk of developing recurrence or progression of diabetic macular edema. PLoS One. 2025 Aug 18;20(8):e0328874. doi: 10.1371/journal.pone.0328874. PMID: 40824925; PMCID: PMC12360533.
- Md. Obaidur Rahman, Sudhir Kumar. A Study on the Visual Outcomes of Cataract Surgery in Diabetic Patients and Assessment of Post-operative Complications Compared to Non-Diabetic Patients. The European Journal of Cardiovascular Medicine. 2025 Feb;15(Iss 2):183-189. doi: 10.5083/ejcm/25-02-22.
- Boned-Murillo A, Fernández-Espinosa G, Orduna-Hospital E, et al. Changes in inner retina thickness and macular sensitivity in patients with type 2 diabetes with moderate diabetic retinopathy. Biomedicines. 2023;11(11):2972. doi: 10.3390/biomedicines11112972.