
Журнал «Здоровье ребенка» Том 21, №2, 2026
Вернуться к номеру
Кардіоензими порівняно з МРТ серця для ранньої діагностики міокардиту в дітей
Авторы: Hussein A. Alsalkhi
Najaf Cardiac Center, Faculty of Medicine, University of Kufa, Kufa, Iraq
Рубрики: Педиатрия/Неонатология
Разделы: Клинические исследования
Версия для печати
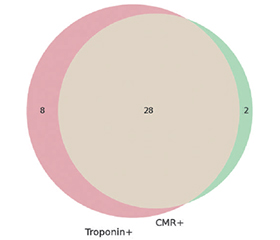
Актуальність. Діагностика міокардиту в дітей залишається складною через неспецифічну клінічну картину й відсутність будь-якого інструменту оцінки. Кардіотропоніни не є специфічними для цього захворювання, а магнітно-резонансна томографія серця (МРТС) забезпечує детальну характеристику тканини міокарда. Мета: визначення діагностичної ефективності високочутливого кардіотропоніну та МРТС за допомогою критеріїв Lake Louise 2018 року в дітей із підозрою на гострий міокардит, а також оцінка додаткової користі поєднаного використання обох тестів. Матеріали та методи. Це проспективне діагностичне дослідження проведене в Кардіологічному центрі провінції Наджаф (Куфа, Ірак) з січня 2024 року до січня 2026 року. Було залучено сто дітей віком від 6 місяців до 16 років із клінічною підозрою на гострий міокардит. Усі пацієнти пройшли серійне визначення високочутливого кардіотропоніну протягом перших 24 годин і стандартизовану МРТС відповідно до критеріїв Lake Louise 2018 року. МРТС використовували як еталонний метод. Були розраховані показники діагностичної точності (ROC-аналіз, тестування узгодженості) та кореляції між рівнем тропоніну й параметрами МРТС. Результати. МРТС підтвердила міокардит у 30 % пацієнтів. Високочутливий тропонін продемонстрував високі чутливість (93,3 %) і негативну прогностичну цінність (96,4 %), але нижчу специфічність (87,1 %) та позитивну прогностичну цінність (77,8 %). МРТС мала високу специфічність (97,1 %) і загальну діагностичну точність. Узгодженість між вимірюванням тропоніну й МРТС була суттєвою (коефіцієнт κ Коена = 0,78). Рівні тропоніну вірогідно корелювали з набряком міокарда, його пошкодженням та ступенем пізнього посилення гадолінієм під час МРТС, але не з фракцією викиду лівого шлуночка. Комбіноване використання тропоніну й МРТС мало 100% чутливість та негативну прогностичну цінність. Висновки. Високочутливий кардіотропонін є корисним методом раннього скринінгу при підозрі на дитячий міокардит, однак сам по собі він не має достатньої специфічності. МРТС із використанням критеріїв Lake Louise 2018 року забезпечує більш точну діагностичну верифікацію. Поєднання обох методів значно підвищує діагностичну ефективність та впевненість у встановленні діагнозу: оптимальною є поетапна стратегія — ранній скринінг тропоніну із подальшим цільовим проведенням МРТС.
Background. Diagnosis of myocarditis in children is still difficult because of nonspecific clinical presentation and lack of any specific tool. Cardiac troponins are not disease-specific and cardiac magnetic resonance imaging (CMR) offers detailed myocardial tissue characterization. This study was designed to determine the diagnostic performance of high-sensitivity cardiac troponin and CMR using the 2018 Lake Louise Criteria (LLC) in children with suspected acute myocarditis, and to evaluate the incremental benefit of both tests used together. Materials and methods. This was a prospective diagnostic study performed at the Najaf Cardiac Center from January 2024 to January 2026. One hundred children (ages 6 months to 16 years) with clinical suspicion of acute myocarditis were enrolled. All patients underwent serial high-sensitivity cardiac troponin testing within the first 24 h and a standardized CMR read based upon the 2018 LLC. CMR was used as the standard of reference. Diagnostic accuracy measures (receiver operating characteristic analysis, agreement testing) and correlations between troponins and CMR parameters were calculated. Results. CMR confirmed myocarditis in 30 % of patients. High-sensitivity troponin demonstrated high sensitivity (93.3 %) and negative predictive value (96.4 %) but lower specificity (87.1 %) and positive predictive value (77.8 %). CMR showed high specificity (97.1 %) and overall diagnostic accuracy. Agreement between troponin and CMR was substantial (Cohen’s κ = 0.78). Troponin levels correlated significantly with myocardial edema, injury, and extent of late gadolinium enhancement on CMR but not with left ventricular ejection fraction. Combined use of troponin and CMR achieved 100 % sensitivity and negative predictive value. Conclusions. High-sensitivity cardiac troponin is a useful early screen for suspected pediatric myocarditis; however, it does not have adequate specificity alone. CMR with the 2018 LLC gives better diagnostic verification. There is significant improvement in diagnostic performance and confidence of troponin screening with targeted CMR translation by using a combined stepwise approach for early troponin screening followed by selective CMR.
міокардит; серцевий тропонін; магнітно-резонансна томографія серця; критерії Lake Louise; діагностична точність; запалення міокарда
myocarditis; cardiac troponin; cardiac magnetic resonance imaging; Lake Louise Criteria; diagnostic accuracy; myocardial inflammation