
Журнал «Травма» Том 27, №3, 2026
Вернуться к номеру
Визначення клінічних фенотипів остеоартриту медіального відділу колінного суглоба шляхом кластерного аналізу
Авторы: O.O. Kostrub (1), R.I. Blonskyi (1, 2), L.O. Kylymniuk (1), O.Yu. Branitskyi (3), V.O. Movchaniuk (4), M.M. Matsipura (3)
(1) - Institute of Traumatology and Orthopedics of NAMSU, Kyiv, Ukraine
(2) - Private Higher Educational Institution “Kyiv Medical University”, Kyiv, Ukraine
(3) - Vinnytsia National Pirogov Memorial Medical University, Vinnytsia, Ukraine
(4) - Medical and Diagnostic Center “Medilux” Ltd, Vinnytsia, Ukraine
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
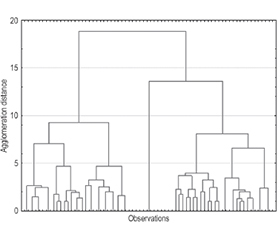
Актуальність. Остеоартрит колінного суглоба є надзвичайно поширеним і гетерогенним захворюванням, що підкреслює необхідність застосування фенотипорієнтованих підходів до стратифікації пацієнтів. Мета: визначити фенотипи остеоартриту медіального відділу колінного суглоба шляхом кластерного аналізу коморбідних характеристик та механічних факторів, пов’язаних із захворюванням. Матеріали та методи. Проведено ретроспективне обсерваційне дослідження даних 70 пацієнтів з остеоартритом медіального відділу колінного суглоба. Оцінювали демографічні, клінічні, коморбідні й механічні фактори. Для узагальнення доменних ознак формували композитні індекси (кількісний показник, розрахований як сума наявних ознак) та бінарні індикатори доменів (наявність домену визначали при виявленнi ≥ 1 ознаки). Фенотипування проводили за допомогою двохетапного кластерного аналізу (метод Варда з подальшим застосуванням алгоритму k-середніх). Міжкластерні відмінності оцінювали з використанням непараметричних статистичних методів. Відмінності вважали статистично значущими при p ≤ 0,05. Результати. У результаті кластерного аналізу ідентифіковано три фенотипи остеоартриту медіального відділу колінного суглоба. Для фенотипу 1 характерно накопичення кардіометаболічних факторів ризику та помірний рівень загальної коморбідності. Фенотип 2 вирізняли найвищі значення індексів коморбідності й більша частота серцево-судинних захворювань. Фенотип 3 обумовлений механічними факторами, пов’язаними із захворюванням, включаючи попередні хірургічні втручання в ділянці ураженого колінного суглоба, за мінімального системного коморбідного навантаження. Висновки. Ідентифіковано три фенотипи остеоартриту медіального відділу колінного суглоба, які відображають різні домінуючі клінічні й патогенетичні домени захворювання, зокрема метаболічний, мультиморбідний та механічний. Отримані дані свідчать про багатовимірну природу остеоартриту колінного суглоба і доцільність фенотипорієнтованої стратифікації пацієнтів.
Background. Knee osteoarthritis is a highly prevalent and heterogeneous disease, emphasizing the need for phenotype-based approaches to patient stratification. Aim: to identify phenotypes of medial knee osteoarthritis based on cluster analysis of comorbid characteristics and mechanical disease-related factors. Materials and methods. A retrospective observational study was conducted using data from 70 patients with medial knee osteoarthritis. Demographic, clinical, comorbid, and mechanical factors were assessed. To summarize domain-specific characteristics, composite indices were constructed (quantitative measures calculated as the sum of present features), as well as binary domain indicators (a domain was considered present if ≥ 1 feature was identified). Phenotyping was performed using a two-step cluster analysis approach (Ward’s method followed by the k-means algorithm). Inter-cluster differences were evaluated using nonparametric statistical methods. Differences were considered statistically significant at p ≤ 0.05. Results. Cluster analysis identified three phenotypes of medial knee osteoarthritis. Phenotype 1 was characterized by the accumulation of cardiometabolic risk factors and a moderate level of overall comorbidity burden. Phenotype 2 demonstrated the highest comorbidity index scores and a greater prevalence of cardiovascular involvement. Phenotype 3 was associated with mechanical disease-related factors, including prior surgical interventions in the affected joint, and was accompanied by minimal systemic comorbidity burden. Conclusions. Three phenotypes of medial knee osteoarthritis were identified, reflecting distinct dominant clinical and pathogenetic domains of the disease, including metabolic, multimorbid, and mechanical ones. These findings support the multidimensional nature of knee osteoarthritis and highlight the relevance of phenotype-oriented patient stratification.
остеоартрит колінного суглоба; кластерний аналіз; фенотипи; коморбідність; персоналізована медицина
knee osteoarthritis; cluster analysis; phenotypes; comorbidity; personalized medicine