Резюме
Актуальність. Мелатонін пов’язаний зі сном, настроєм, репродуктивною функцією, розвитком пухлин і старінням. У той же час інформації про важливість мелатоніну для фізіології людини недостатньо. Хронічні проблеми зі сном, стрес, втома, дратівливість, сплутаність свідомості, напруження й симптоми депресії можуть спостерігатися при дефіциті мелатоніну. Подібного дослідження в літературі немає, тому метою дослідження було вивчення зв’язку між рівнем мелатоніну і релігійною орієнтацією, рівнем депресії і якістю сну студентів медсестринського та інших відділень. Матеріали та методи. Це перехресне дослідження проводилося з квітня 2019 року по квітень 2020 року. Цільовою популяцією дослідження були 1200 учасників, які навчаються на другому курсі. Це сприяло отриманню однорідності параметрів стресу, сну й мелатоніну. Вибірка становила 145 осіб, які взяли подальшу участь у дослідженні. Для збору даних використовували описову інформаційну форму, шкали релігійної орієнтації, депресії Бека та індекс якості сну Піттсбурга (PSQI). Результати. Встановлено, що рівень мелатоніну в студентів становив 0,79 ± 0,52 пг/мл, загальний середній бал за шкалою якості сну становив 7,24 ± 3,35, за шкалою депресії Бека — 16,40 ± 10,84 і за шкалою релігійної орієнтації — 47,41 ± 6,05. Було визначено, що якість сну була «поганою», встановлено помірно виражений депресивний стан, а рівень мелатоніну був нижче за норму. Висновки. Оскільки загальна оцінка якості сну студентів перевищувала 5, встановлено, що якість сну була «поганою». У групі обстежених спостерігався помірно виражений стан депресії, учасники вказували на помірно виражену релігійну орієнтацію. У дослідженні, де за стандарт було прийнято 0,90, було виявлено, що рівень мелатоніну перебував нижче за референсні значення. У подальшому рекомендується проводити дослідження в більших за чисельністю групах.
Background. With insufficient information about the importance of melatonin in human physiology, this hormone is known to be associated with sleep, mood, reproduction, tumor development, and aging. Chronic sleep problems, stress, fatigue, irritability, confusion, tension, and depressive symptoms can be observed in melatonin deficiency. There is no such study in the literature and it is thought to shed light on the literature. The purpose of the study is to examine the relationship between melatonin level and religious orientation, depression level, and sleep quality of students in nursing and different department. Materials and methods. This cross-sectional study was conducted between April 2019 and April 2020. The target population of the study consisted of 1200 students who studying in 2nd grade to ensure harmony and homogeneity in stress, sleep, and melatonin parameters. The sample of the study consisted of 145 individuals who accepted to participate in the study among the 2nd-grade students. Descriptive Information Form, Religious Orientation Scale, Beck Depression Inventory, and Pittsburg Sleep Quality Index (PSQI) scale were used to collect research data. Results. According to the findings obtained from the study, it was determined that the melatonin level of the students was 0.79 ± 0.52 pg/ml, the total score mean of the Sleep Quality Scale was 7.24 ± 3.35, the Beck Depression Inventory was 16.40 ± 10.84 and the Religious Orientation Scale was 47.41 ± 6.05. It was determined that their sleep quality was “bad”; moderately depressed and religious orientation and the melatonin level was below normal. Conclusions. Since the sleep quality total score of the students was above 5, it was determined that their sleep quality was “bad”. It was found that the group was moderately depressed and had a moderate religious orientation. In the study where the standard was accepted as 0.90, it was found that the melatonin level was below normal. It is recommended that the study be conducted in larger groups.
Introduction
In addition to being a reversible state of unconsciousness, sleep is not only a state of inactivity that allows the body to rest but an active regeneration period that prepares the whole body for life [1]. It has been reported that people who sleep less have more difficulty during the day than those who sleep well, have more difficulty performing functions during the day, and experience more tension and depression [2]. It is known that sleep problems are common among university students and their sleep quality is poor. In the studies on students it has been reported that their time to go to bed to sleep is irregular, they sleep insufficiently, their sleep quality is poor, they frequently use alcohol and even non-prescription drugs to regulate their sleep, and use stimulants to stay awake [3].
It is also reported that students experience problems such as fatigue, anxiety, and depression as a result of sleeplessness [4]. Depression, which is one of the most common mental illnesses in society and accepted as the “common cold” of psychiatry, is briefly defined as the state of collapse that develops after genetic, environmental, or hormonal disorders [5]. In psychiatry, if the above-defined mood lasts long and its negative effects on the social, individual, or professional life of the person are noticeably severe, this is considered a mental illness [6].
People sometimes turn to religion as a remedy in case of depression [7]. As O. Gürsu puts it, religion has both harms and benefits, and the effect of religion on mental health can vary depending on the type and definition of religion, health and happiness criteria, individual differences and personality structures, context and situation, and the level of integration with the individual’s religion [8]. Religion contributes positively to mental health in terms of individuals’ adaptation both individually and with their social environment, and also in terms of giving spiritual support, consolation, and hope to believers in stressful and troubled situations and even making their pain meaningful [7]. However, it is not possible to say that this is always the case when it comes to religiosity and not religion. This is because, just as different forms of religiosity emerge when religion comes into contact with the human sphere, religiosity is not a one-dimensional phenomenon [9].
We can state that there are almost no studies on the relationship between neuroscience-religion and psychological well-being in our country. With insufficient information about the importance of melatonin in human physiology, this hormone is known to be associated with sleep, mood, reproduction, tumor development, and aging. Melatonin is located in the pineal gland, a well-hidden region in the brain called the third eye in Indian philosophy. Indeed, one of the functions of the pineal gland it functions as a kind of natural clock by responding to light and dark changes [10]. Therefore, chronic sleep problems, stress, fatigue, irritability, confusion, tension, and depressive symptoms can be observed in melatonin deficiency [11]. There is no such study in the literature and it is thought to shed light on the literature.
Materials and methods
Study design
This cross-sectional study was conducted between April 2019 and April 2020 with 2nd-year students. The target population of the study consisted of 1200 students who studying in 2nd grade to ensure harmony and homogeneity in stress, sleep, and melatonin parameters. The sample of the study consisted of 145 individuals who accepted to participate in the study among the 2nd-grade students.
Data collection
Descriptive Information Form, Religious Orientation Scale, Beck Depression Inventory, and Pittsburg Sleep Quality Index (PSQI) scale were used to collect research data. Researchers visited the departments on the days and hours at the institutions where the study was conducted deemed appropriate, explaining the purpose of the research, and obtaining verbal permission from those who voluntarily accepted to participate in the study, the questions in the questionnaire were read to the individuals and filled in line with their answers (average 10–15 minutes). Then, 2 cc of blood from the students was taken into ETDA-containing hemogram tubes and centrifuged. Centrifuged samples were stored at appropriate temperatures in Central Research Laboratory until they reached a sufficient number. After the sufficient number was reached, solutions were prepared according to the melatonin kit protocol and measurements were made.
Data collection tools
Introductory Information Form: It consists of questions created by researchers and including introductory features from students.
Religious Orientation Scale: It was developed by A. Onay (2000) to determine the extent of religion in people’s thoughts, behaviors, and feelings [9]. The scale contains 18 Likert-type items, of which twelve are plain and six are reverse-encoded. The scale has three sub-dimensions: thought, behavior, and emotion. The scale is answered as Never, Rarely, Often, Every Time. The upper and lower score limits of the scale are the lowest is 18; the highest is 72. The score obtained from the scale increased to 72 indicates the level of religious orientation rising and decreased to 18 also shows the decreasing level of religious orientation. Cronbach Alpha reliability coefficient of the scale is 0.95 [9]. In our study, the Cronbach Alpha reliability coefficient was found to be 0.68.
Beck Depression Inventory: It is a 21-item self-report scale developed by A.T. Beck et al. (1961) to measure the depression symptom level [12]. Each item is scored between 0 and 3, and the total score varies between 0 and 63. High scores indicate that depression symptom severity increased. Turkish adaptation study was done by N. Hisli (1989) [13]. In the study, the sum of the scores of the 4, 12, and 21 items of the Beck Depression Inventory was calculated as the anhedonia score, and the sum of the scores of the 5, 11, 12, 16, and 21 items was calculated as the melancholy score and included in the analyzes as the BDI subscale scores. In the study, 17 points, which is the cut-off score defined for the diagnosis of major depression in N. Hisli’s (1989) study, was used as a diagnostic indicator. The Cronbach alpha coefficient of the scale was found to be 0.80 [13]. In our study, the Cronbach Alpha reliability coefficient was found to be 0.90.
Pittsburg Sleep Quality Index (PSQI)
PSQI was developed by D.J. Buysse et al. in 1989 and has been shown to have sufficient internal consistency, retest reliability, and validity [14]. In our country, the reliability and validity of the scale were carried out by M.Y. Ağargün et al. in 1996 [15]. The PSQI, which evaluates the sleep quality of the individual for the last month, includes a total of 24 questions. The 18 items included in the scoring are grouped into 7 component scores. These components provide information about subjective sleep quality (component 1), sleep latency (component 2), sleep duration (component 3), habitual sleep efficiency (component 4), sleep disturbance (component 5), use of sleeping pills (component 6), and daytime sleep dysfunction (component 7). Each question is evaluated with a number from 0 to 3. The sum of the scores of the seven components gives the total PSQI score. The total PSQI score takes a value between 0–21. Sleep quality of those with a total score of 5 or less is “good”; Sleep quality of those over 5 is evaluated as “bad”. One of the most important factors affecting sleep quality is sleep duration. The Cronbach Alpha internal consistency coefficient of the scale was found to be 0.80 [15]. Cronbach Alpha reliability coefficient was found 0.78 in our study.
Analysis of the data
IBM SPSS V-25 program was used in the statistical analysis of the study. Analyzed is made with SPSS-25 program installed in a university in Turkey. In the research, descriptive features are presented with number (n) and percentage (%). Continuous variables are specified with their mean, standard deviation, minimum and maximum values. In the process of analyzing the data, necessary normality tests were performed (Kolmogorov-Smirnov test) and it was determined that the data did not show a normal distribution. Mann-Whitney U test was used for binary groups in data that did not show normal distribution. Kruskal-Wallis test was also used for data with more than two continuous variables and normally distributed. Spearman correlation test was used to determine the linear relationship between variables and severity of the relationship. P value of < 0.05 was considered statistically significant.
Ethical principles
Ethical approval was obtained from the Scientific Research Ethics Committee and written permission was obtained from the institutions where the study would be conducted. The necessary explanations were made to the individuals included in the study, and verbal permission was obtained from those who wanted to participate in the study.
Results
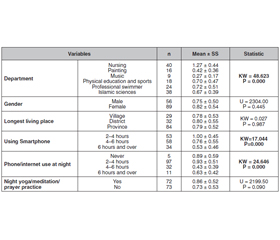
It was determined that 27.6 % of the students participating in the study studied nursing, 61.4 % were women, 57.9 % lived in the district for the longest time, 40.0 % used an average of 4–6 hours, 66.9 % had telephone/internet for 2–4 hours at night, 50.3 % of them did not practice night yoga/meditation/prayer. The mean age of the group was 21.27 ± 2.015 years, the total score mean of the Sleep Quality Scale (PSQI) was 7.24 ± 3.35, the melatonin level was 0.79 ± 0.52 pg/ml, the Beck Depression Inventory (BDI) total score mean was 16.40 ± 10.84, and the total score mean of the Religious Orientation Scale (ROS) was found to be 47.41 ± 6.05 (Table 1).
The mean score of the Sleep Quality Scale (PSQI) was found to be statistically significantly higher in those who study at the painting department, those who use phones for more than 6 hours, and those who use telephone/internet at night for more than 6 hours (p < 0.05) (Table 2).
The Beck Depression Inventory (BDI) total score mean was found to be statistically significantly higher in those who study the painting department, women, those who use the phone for more than 6 hours, those who use the phone/internet for more than 6 hours at night, and those who do not practice yoga/meditation/prayer at night (p < 0.05) (Table 3).
The total score mean of the Religious Orientation Scale (ROS) was found to be statistically significantly higher in those who study Islamic sciences, women, and those who practice yoga/meditation/prayer at night (p < 0.05) (Table 4).
The mean score of melatonin level was found to be statistically significantly higher in those studying the nursing department, those who used phones for 2–4 hours, and those who used telephone/internet for 2–4 hours at night (p < 0.05) (Table 5).
A statistically significant negative correlation was found between the Beck Depression Inventory and the Sleep Quality Scale total score and the melatonin level (p < 0.05). There was no statistically significant relationship between the total score of the Religious Orientation Scale and the melatonin level (p > 0.05). A statistically significant positive correlation was found between the total score of the Sleep Quality Scale and the total score of the Beck Depression Inventory (p < 0.05). A statistically significant negative correlation was found between the total score of the Religious Orientation Scale and the total score of the Sleep Quality Scale and Beck Depression Inventory (p < 0.05) (Table 6).
Discussion
In the literature, there is no study to determine the relationship between melatonin level and religious orientation, depression level, and sleep quality, and to add new findings to the literature in line with our study, the relationship between melatonin level and religious orientation, depression and sleep quality of university students was examined.
A statistically significant negative correlation was found between the Beck Depression Inventory total score and melatonin level (p < 0.05). It was found that the higher the depression level, the lower the melatonin level. It has been determined that many pharmacological antidepressants stimulate melatonin secretion by increasing the happiness hormone serotonin. This highlights the link between an increase in melatonin production and the benefit seen from the treatment. Studies have shown that there is a decrease in melatonin release associated with the increase in cortisol, known as the stress hormone, in depression [16]. According to the photoperiodic hypothesis, long nights, or short days in the winter season cause seasonal affective disorder (SAD) [17]. The main reason for this is the body’s release of melatonin. This hypothesis is supported by the fact that this picture goes into remission spontaneously in the summer, progresses in the form of recurrent depression attacks in autumn or winter, and that SAD can be treated with bright light [18]. Studies show that melatonin used for treatment regulates the sleep pattern in patients with depression and causes regression of depression symptoms [18].
There was no statistically significant relationship between the total score of the Religious Orientation Scale and the melatonin level (p > 0.05). When the literature is reviewed, it has been found that there is a close relationship between religion and melatonin [19–23]. This situation in our study is thought to be caused by the fact that melatonin is affected by many factors such as stress and sleep as well as religion. When the literature is reviewed, it is understood that the pineal gland (also known as the pineal gland) plays a leading role in the mystical pleasures and ecstasies experienced by humans, the trance state, the work of spiritual grace, unusual leaps of consciousness and psychic current jumps. The common point between meditation, yoga, dhikr studies, incense and harmaline (Peganum harmala) chemical that has a melatonin effect on human beings (hanged on the entrance door of houses in Anatolia), mystical dances and music, frankincense and ritual drinks. All these different elements stimulate the pineal gland or produce results similar to the hormones secreted by this gland [24]. We can explain the high level of oscillation of the pineal gland in these places when Muhammad chose to retreat to a dark cave and took his command there, and Moses went up the mountain to speak to God [20]. The fact that priests chose the time of waking at night to communicate with God and preferred the night to meditate and pray in the Far Eastern traditions showed that they preferred the time when melatonin was high in their religious orientation [23]. There is also great evidence that the pineal gland from which melatonin is secreted is important in different religions. When we look at these concrete pieces of evidence, the pineal gland, which comes from the root of “Pinecone” in connection with the Latin “pine”, is in a conical shape and is seen as the third eye. To show the value they give to the pineal gland, the pope's scepter has a conifer figure. There is a cone statue in the middle of the Vatican, which is considered sacred, and “Pine Cone Square”, which is considered very sacred by the Vatican, is a square where the world’s largest pineal gland symbol is displayed.
In Indian Philosophy, it is the crown of the 7 Chakras and the place where the soul is inhabited and is considered the core of the soul. In ancient societies, especially the Egyptians and Romans, they knew the benefits of the pineal gland and symbolized it with the eye symbol in their broad symbology. Is it a coincidence that the Sumerians depict their God Anunnaki with a cones in their hands, in Ancient Greece the Wine God Dionysus depicts a conifer on his staff just like the Pope, the symbol of cones in ancient Buddha statues in the Far East, the domes of some ancient temples in India are in the form of cones, all ancient cultures from Cambodia to South America, from the Romans to the Olmecs attach great importance to the cones symbol, that the entrance to the Aachen Cathedral in Germany is cone, the body of the Eagle, one of the Nazis’ symbols, and the spear figures on Hitler’s desk have a cones on the end, the Gherkin Building Built in the Heart of London, the Indian Goddess Shiva’s hair, the F.C Augsburg Football Club logo belonging to Augsburg, the Masonic Lodge to which Mozart and his family are members, and the cone on the staff of Osiris, Egypt’s immortal god of life, the symbol of cones in the Masonic lodge, “Esma-ül Hüsna”, which describes the 99 names of Allah in Islam, is sometimes engraved on me–tal cones? Although its philosophical dimension is a larger subject of discussion and argument, this cocoon-like pineal gland, namely the “Third Eye”, has been a secret since ancient times; Cyclops in the Dede Korkut Stories, Egegöz, Yalgizgöz in Central Asian myths; In Roman-Greek Mythology, the common feature of creatures that appear in the cultures of many civilizations, such as the Cyclopean, the all-seeing eye of the sun god Ra of Egypt, is the eye in the middle of the forehead. That eye is perhaps the cone-shaped pineal gland [21, 22].
A statistically significant negative correlation was found between the total score of the Sleep Quality Scale and melatonin level (p < 0.05). It was found that as the mean score of sleep quality increased, the melatonin level decreased. The increase in the mean score of sleep quality indicates that the sleep quality is poor, and this has been found to reduce the melatonin level. When we look at the changes in melatonin during the day, the nocturnal concentrations of melatonin in the blood and cell are 3–10 times higher than during the day. The secretion of melatonin usually starts at 09:00–10:00 p.m. and reaches its maximum between 02:00–04:00 a.m. hours [25]. Similar results were found in many studies in the literature [26–28].
A positive statistically significant relationship was found between the total score of the Sleep Quality Scale and the Beck Depression Inventory (p < 0.05). A similar result has been found in the literature [29].
A statistically significant negative correlation was found between the total score of the Sleep Quality Scale and the total score of the Religious Orientation Scale (p < 0.05). This suggests that individuals practice more nighttime prayers due to their religious orientation, and it is relevant that interruption of night sleep improves sleep quality.
A statistically significant negative correlation was found between the Beck Depression Inventory total score and the Religious Orientation Scale total score (p < 0.05). Gursu states that religion can increase the self-confidence of the person and the determination to fight against the problems so that religion has an important function in coping with situations that cause anxiety, distress, and depression-like disasters, illness, death, etc. [8].
Conclusions
Since the sleep quality total score of the students was above 5, it was determined that their sleep quality was “bad”. It was found that the group was moderately depressed and had a moderate religious orientation. In the study where the standard was accepted as 0.90, it was found that the melatonin level was below normal. It is recommended that the study be conducted in larger groups.
Received 15.06.2022
Revised 21.07.2022
Accepted 01.08.2022

/28.jpg)
/29.jpg)
/30.jpg)