Introduction
Urolithiasis affects 1 of 11 people in the USA, having a slightly higher prevalence in men [1]. The typical presentation is colicky flank pain alongside nausea, vomiting and fever [1]. Most calculi will pass spontaneously though, the likelihood of this occurring decreases with calculus size [1]. However, despite the relatively high prevalence of urolithiasis, few cases of retrograde migration have been reported. We present a rare case of retrograde urolithiasis migration.
Case report
A 47-year-old woman presented with left flank pain to the radiology department following a referral from her general practitioner to exclude urolithiasis. The patient had presented with similar symptoms two years previous, at which point a single non-obstructive kidney stone of 2 mm was found within the left renal calyx during a CT (Computed Tomography) examination (Figure 1).
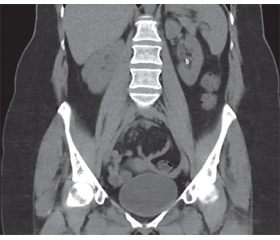
Upon this occasion, the pain had fluctuated since its first appearance four days prior and was coupled with white blood cells and red blood cells in the urine. A CT-examination demonstrated a 3 mm calculus located in the left proximal ureter with mild hydronephrosis, and no calculus within the kidney (Figure 2).
The patient was treated conservatively before subsequently presenting 11 days later for a follow up CT-exam to verify that the calculus had been eliminated, the pain having subsided in the meantime, leading the clinician to suspect that natural elimination had occurred. Surprisingly, the 3 mm calculus was once again observed, in the inferior renal calyx, with concomitant resolution of the hydronephrosis (Figure 3). We therefore hypothesize upward migration.
An abdominal x-ray was performed three days later, finding that the calculus was radiopaque and remained in the renal calyx.
Discussion
One could hypothesise that the migrating calculus seen in the lumbar ureter had been eliminated and that a second calculus, which had appeared in the meantime, was seen on the follow-up CT examination in the left inferior calix. This would raise two possibilities: first, that we would have missed a 3 mm calculus in the kidney on the first CT examination, or second that a new calculus had formed within the intervening 11 days.
It is improbable that there was a second, missed, kidney stone on the initial CT-exam given that CT technique has a reported sensitivity of up to 99 % with regards to the detection of kidney stones [2]. It is also improbable that a new 3 mm calculus formed within 11 days, as the average recurrence time for new symptomatic urolithiasis is over a year [3]. Furthermore, we know that in this patient the calculus took 2 years to grow from 2 to 3 mm in diameter, making the novel calculus hypothesis yet more improbable [3]. These facts make us confident that there was only a single kidney stone in this patient. Due to the improbability of both above-mentioned hypotheses, we therefore postulate that the calculus seen in the lumbar ureter had migrated upwards.
Although urolithiasis is a relatively common occurrence, fewer than 10 cases of retrograde urolithiasis migration have been documented once it has entered the ureter. The first documented case in English literature dates from 2015 in Bahrain, with a few cases in the Middle East and India documented afterwards [4–7]. Of the previously reported cases, only Fatallah et al reported relatively little distal migration of the urolithiasis before it was subsequently found to have migrated back into the calyx, whereas the other reports detail the calculus having migrated to the vesicoureteral junction before beginning its retrograde migration [4–7]. The previous papers report intervals of 3 days to around 2 weeks between the onset of pain and its subsequent resolution, at which point it was assumed that the calculus had been spontaneously passed, as was the case in our patient, before it was discovered to have migrated to kidney [4–7].
Previous studies have shown that, once the calculus is within the ureter, the normal anterograde peristalsis of the ureter is disturbed [8]. Interestingly, the peristalsis becomes retrograde in the majority of cases when the calculus is in the proximal ureter, followed by a majority of uncoordinated waves once the calculus is in the distal ureter [8]. Retrograde peristalsis has also been observed in pig models after prolonged stenting, suggesting that foreign bodies, such as an impacted calculus, may be the inducing factor [9]. This theory is backed by evidence from Davenport et al who found that stretch and irritation from calculi resulted in abnormal peristalsis, thus building on a 1973 study which demonstrated abnormal peristalsis following acute or chronic obstruction [10, 11]. Furthermore, retrograde migration of urolithiases have also been recorded in both cats and dogs, lending further credence to the supposition that this is a natural phenomenon present across multiple species [12].
To summarise, there are many reports in the literature of ureter peristalsis being disturbed by a foreign object, with a propensity for retrograde peristalsis if the object is in the proximal ureter. Additionally, the retrograde peristalsis has been documented multiple times in vivo in both human and animal models. It therefore seems highly likely that, since the in vivo observations correlate with the expected outcome of the laboratory findings, that retrograde urolithiasis migration is due to a coordinated physiological response and not merely coincidence.
With regard to the evolutionary reason for the development of such a physiological response, one could theorise that, given the resultant morbidity and mortality in untreated urolithiasis cases, this mechanism might exist to move the calculi back into the kidney where they can remain asymptomatic [13, 14]. However, in the absence of further evidence to prove the evolutionary pressure for this to develop, this remains merely conjecture.
Given the relatively high incidence of urolithiasis it therefore seems unlikely that retrograde migration is so rare, even though it has only been documented a handful of times. We therefore speculate that ureteric calculi, which subsequently spontaneously undergoes retrograde migration, may be an explanation for relatively short-lived flank pain in patients who are found to have nephrolithiasis later but who did not undergo immediate imaging during the painful episode, resulting in the phenomenon going undocumented.
Conclusion
Retrograde urolithiasis migration as in this case is a rare, but probably underreported, phenomenon where a calculus that has begun its migration within the ureter undergoes retropulsion back into the renal calyx. Building on the previous reports and studies, we suggest that this may be a natural phenomenon aiming to protect the patient from potentially deadly impaction of the urolithiasis by returning it to the relative safety of the renal calyx.
Acknowledgments: We would like to thank Dr Emily Antonovics for providing feedback regarding legibility and clarity of the manuscript prior to submission.
Received 06.07.2022
Revised 20.07.2022
Accepted дата 03.08.2022
Список литературы
1. Thakore P., Liang T.H. Urolithiasis. StatPearls Publishing, 2022.
2. Rodger F., Roditi G., Aboumarzouk O.M. Diagnostic Accuracy of Low and Ultra-Low Dose CT for Identification of Urinary Tract Stones: A Systematic Review. Urol. Int. 2018. 100. 375-385. https://doi.org/10.1159/000488062.
3. Levi O., Tsivian A., Baniel J. et al. The Correlation Between Renal Stone Composition and the Risk of Stone Recurrence (Mp13-15 ). J. Urol. 2018. 199. https://doi.org/10.1016/j.juro.2018.02.487.
4. Khan Z., Yaqoob A.A., Bhatty T.A. Spontaneous retrograde migration of ureterovesical junction stone to the kidney; first ever reported case in the English literature in human. Urol. Ann. 2016. 8. 229. https://doi.org/10.4103/0974-7796.176869.
5. Patil S., Jebaraj A., Kundargi V.S., Patil B.S. Spontaneous retrograde migration of mid ureteric calculus into the kidney: First ever report from India. Int. J. Surg. Sci. 2020. 4. 272-274. https://doi.org/10.33545/SURGERY.2020.V4.I1E.346
6. Miah S., Connor M.J., Wiseman O., Shah N. Retrograde migration of a vesicoureteric junction calculus: A potential pitfall of the noncontrast limited pelvic computerized tomography. Urol. Ann. 2021. 13. 80-82. https://doi.org/10.4103/UA.UA_25_20.
7. Fallatah M., Tahaineh S., Mughli R.A., Fallatah S.M. Upward migration of a ureteric stone in a military trainer: a case report. Res. Reports Urol. 2017. 9. 15. https://doi.org/10.2147/RRU.S124200.
8. Irina M., Lubov K. Ureteric Function and Upper Urinary Tract Urodynamics in Patients with Stones in Kidney and Ureter. In: Kommu S. (ed.) Evolving Trends in Urology. InTech, London, 2012. Р. 37-68.
9. Kinn A.C., Lykkeskov-Andersen H. Impact on ureteral peristalsis in a stented ureter. An experimental study in the pig. Urol. Res. 2002. 304. 30. 213-218. https://doi.org/10.1007/S00240-002-0258-1.
10. Rose J., Gillenwater J. Pathophysiology of ureteral obstruction. Am. J. Physiol. Content. 1973. 225. 830-837. https://doi.org/10.1152/ajplegacy.1973.225.4.830.
11. Davenport K., Timoney A.G., Keeley F.X. The Role of Ureteral Relaxation in the Promotion of Stone Passage. In: AIP Conference Proceedings. AIP, 2007. Р. 243-252.
12. Dalby A.M., Adams L.G., Salisbury S.K., Blevins W.E. Spontaneous retrograde movement of ureteroliths in two dogs and five cats. J. Am. Vet. Med. Assoc. 2006. 229. 1118-1121. https://doi.org/10.2460/JAVMA.229.7.1118.
13. Kum F., Mahmalji W., Hale J. et al. Do stones still kill? An analysis of death from stone disease 1999–2013 in England and Wales. BJU Int. 2016. 118. 140-144. https://doi.org/10.1111/BJU.13409.
14. Keoghane S., Walmsley B., Hodgson D. The natural history of untreated renal tract calculi. BJU Int. 2010. 105. 1627-1629. https://doi.org/10.1111/J.1464-410X.2010.09389.X.

/97.jpg)
/98.jpg)