
Журнал «Практическая онкология» Том 6, №1, 2023
Вернуться к номеру
Аденокарцинома порожньої кишки при PMS2-асоційованому синдромі Лінча. Огляд літератури та клінічний випадок
Авторы: Кропельницький В.О., Зайвелєва Ю.І., Кондратенко Б.М.
Національний інститут хірургії та трансплантології імені О.О. Шалімова НАМН України, м. Київ, Україна
Рубрики: Онкология
Разделы: Справочник специалиста
Версия для печати
Пухлини тонкої кишки — це рідкісна патологія. За даними українського канцер-реєстру, вони становлять 0,2 % усіх злоякісних новоутворень. Аденокарциноми становлять 40,9 % усіх пухлин цієї локалізації. Частіше вони виявляються у дванадцятипалій кишці, рідше у здухвинній, і найбільш рідкісна локалізація — порожня кишка (5,9 %). Аденокарцинома тонкої кишки може бути пов’язана із синдромом Лінча. Синдром Лінча — гетерогенна патологія, зумовлена гермінальними мутаціями у генах, що кодують білки MMR-системи: MLH1, PMS2, MSH2, MSH6, EPCAM. Частіше при цьому синдромі зустрічаються пухлини колоректальної зони, ендометрія, шлунка, проте рідше можуть виявлятися пухлини багатьох локалізацій, у тому числі тонкої кишки. Залежно від того, у якому саме гені відбулася мутація, прояви синдрому Лінча можуть варіювати. PMS2-асоційовані випадки характеризуються більш старшим віком виникнення пухлин, меншою пенетрантністю, меншою кількістю випадків колоректального раку та раку ендометрія. Це призводить до того, що такі пацієнти не підпадають під класичні клінічні критерії діагностики синдрому Лінча. Усі випадки пухлин при синдромі Лінча характеризуються мікросателітною нестабільністю. Наявність мікросателітної нестабільності впливає на прийняття рішення про післяопераційну тактику лікування. У нашій роботі наведено огляд літератури та клінічний випадок діагностики та лікування аденокарциноми порожньої кишки у пацієнта з PMS2-асоційованим синдромом Лінча. Пропонуємо тестувати усі випадки аденокарцином тонкої кишки на наявність мікросателітної нестабільності.
Small intestine tumors are rare pathology. According to the Ukrainian cancer registry, they account for 0.2 % of all malignant neoplasms. Adenocarcinomas make up 40.9 % of all tumors of this location. They are more often found in the duodenum, less often in the ileum, and the rarest localization is the jejunum (5.9 %). Small bowel adenocarcinoma may be associated with Lynch syndrome. Lynch syndrome is a heterogeneous pathology caused by germline mutations in the genes encoding the MMR-system proteins: MLH1, PMS2, MSH2, MSH6, EPCAM. Colorectal, endometrial and gastric cancers occur more often in this syndrome; tumors of many other locations, including the small intestine, can be detected less often. Depending on the specific gene in which the mutation occurred, Lynch syndrome manifestations may vary. PMS2-associated cases are characterized by an older age of tumor diagnosis, lower penetrance, fewer cases of colorectal and endometrial cancer. This leads to the fact that such patients do not meet classic clinical criteria for Lynch syndrome diagnosis. All cases of tumors in Lynch syndrome are characterized by microsatellite instability. The presence of microsatellite instability affects the decision making about postoperative management. In our work, we present a literature review and a clinical case of diagnosis and treatment of jejunal adenocarcinoma in a patient with PMS2-associated Lynch syndrome. We suggest testing all small bowel adenocarcinoma cases for the presence of microsatellite instability.
рак тонкої кишки; аденокарцинома порожньої кишки; синдром Лінча; мікросателітна нестабільність; PMS2
small bowel cancer; jejunal adenocarcinoma; Lynch syndrome; microsatellite instability; PMS2
Вступ
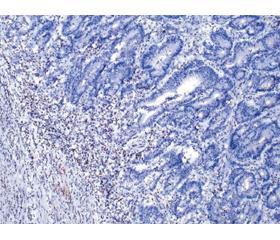
Клінічний випадок
/23.jpg)
Обговорення
Висновки
- Fedorenko Z.P., Hulak L.O., Mykhailovych Yu.Y., et al. Cancer in Ukraine, 2019–2020. Incidence, mortality, prevalence and other relevant statistics. Bulletin of the National Cancer Registry of Ukraine. 2021. 22. Available at http://ncru.inf.ua/publications/BULL_22/index_e.htm
- National Cancer Institute. Cancer stat facts: small intestine cancer, 2022. Surveillance, Epidemilogy, and End Results Program. Available at: https://seer.cancer.gov/statfacts/html/smint.html. Accessed December 5, 2022.
- Mohammed A., Trujillo S., Ghoneim S., et al. Small Bowel Adenocarcinoma: a Nationwide Population-Based Study [published online ahead of print, 2022 Jan 10]. J. Gastrointest. Cancer. 2022. doi: 10.1007/s12029-021-00653-7.
- Pedersen K.S., Raghav K., Overman M.J. Small Bowel Adenocarcinoma: Etiology, Presentation, and Molecular Alterations. J. Natl. Compr. Canc. Netw. 2019. 17(9). 1135-1141. doi: 10.6004/jnccn.2019.7344.
- Li X., Liu G., Wu W. Recent advances in Lynch syndrome. Exp. Hematol. Oncol. 2021. 10. 37. https://doi.org/10.1186/s40164-021-00231-4.
- Yang G., Zheng R.Y., Jin Z.S. Correlations between microsatellite instability and the biological behaviour of tumours. J. Cancer Res. Clin. Oncol. 2019. 145(12). 2891-2899. doi: 10.1007/s00432-019-03053-4.
- Lynch H.T., Lanspa S., Shaw T., et al. Phenotypic and genotypic heterogeneity of Lynch syndrome: a complex diagnostic challenge. Fam. Cancer. 2018. 17(3). 403-414. doi: 10.1007/s10689-017-0053-3.
- Blount J., Prakash A. The changing landscape of Lynch syndrome due to PMS2 mutations. Clin. Genet. 2018. 94(1). 61-69. doi: 10.1111/cge.13205.
- Ten Broeke S.W., van der Klift H.M., Tops C.M.J., et al. Cancer Risks for PMS2-Associated Lynch Syndrome [published correction appears in J. Clin. Oncol. 2019 Mar 20. 37(9). 761]. J. Clin. Oncol. 2018. 36(29). 2961-2968. doi: 10.1200/JCO.2018.78.4777.
- Sanne W. ten Broeke, Mar Rodríguez-Girondo, Manon Suerink, et al. The Apparent Genetic Anticipation in PMS2-Associated Lynch Syndrome Families Is Explained by Birth-cohort Effect. Cancer Epidemiol. Biomarkers Prev. 2019 June 1. 28 (6). 1010-1014. https://doi.org/10.1158/1055-9965.EPI-18-0576.
- Suerink M., Kilinç G., Terlouw D., et al. Prevalence of mismatch repair deficiency and Lynch syndrome in a cohort of unselected small bowel adenocarcinomas. J. Clin. Pathol. 2021. 74(11). 724-729. doi: 10.1136/jclinpath-2020-207040.
- Xia M., Singhi A.D., Dudley B., et al. Small Bowel Adenocarcinoma Frequently Exhibits Lynch Syndrome-associated Mismatch Repair Protein Deficiency But Does Not Harbor Sporadic MLH1 Deficiency. Appl. Immunohistochem. Mol. Morphol. 2017. 25(6). 399-406. doi: 10.1097/PAI.0000000000000389.
- Latham A., Shia J., Patel Z., et al. Characterization and Clinical Outcomes of DNA Mismatch Repair-deficient Small Bowel Adenocarcinoma. Clin. Cancer Res. 2021. 27(5). 1429-1437. doi: 10.1158/1078-0432.CCR-20-2892.
- Sun B.L. Current Microsatellite Instability Testing in Management of Colorectal Cancer. Clin. Colorectal Cancer. 2021. 20(1). e12-e20. doi: 10.1016/j.clcc.2020.08.001.
- National Comprehensive Cancer Network. Small Bowel Adenocarcinoma (Version2.2022). https://www.nccn.org/professionals/physician_gls/pdf/small_bowel.pdf. Accessed November 10, 2022.
- Li J., Wang Z., Liu N., Hao J., Xu X. Small bowel adenocarcinoma of the jejunum: a case report and literature review. World J. Surg. Oncol. 2016. 14(1). 177. Published 2016 Jul 4. doi: 10.1186/s12957-016-0932-3.
- Mujeeb Ullah A., Jaysing A., Hashmi H.R., et al. Primary small bowel adenocarcinoma with loss of nuclear expression of PMS2 after resection of mucinous cholangiocarcinoma. J. Surg. Case Rep. 2022. 2022(1). rjab628. Published 2022 Jan 31. doi: 10.1093/jscr/rjab628.
- Patel J., Zhang H., Sohail C.S., et al. Jejunal Adenocarcinoma: A Rare Cause of Small Bowel Obstruction. Cureus. 2022. 14(1). e21195. Published 2022 Jan 13. doi: 10.7759/cureus.2119.
- Pereira R., Tojal A., Gomes A., et al. Adenocarcinoma of the jejunum: management of a rare small bowel neoplasm. J. Surg. Case Rep. 2021. 2021(4). rjab124. Published 2021 Apr 22. doi: 10.1093/jscr/rjab124.