
Журнал «Здоровье ребенка» Том 19, №1, 2024
Вернуться к номеру
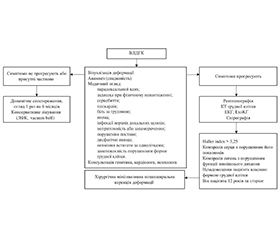
Етапність обстеження, діагностики та корекції вродженої лійкоподібної деформації грудної клітки у дітей
Авторы: Камінська М.О., Дігтяр В.А.
Дніпровський державний медичний університет, м. Дніпро, Україна
Рубрики: Педиатрия/Неонатология
Разделы: Справочник специалиста
Версия для печати
Вроджена лійкоподібна деформація грудної клітки (ВЛДГК) — найчастіша вада розвитку грудино-реберного комплексу, створює косметичний дефект, впливає на психоемоційний стан та викликає функціональні розлади органів середостіння та легень. Спочатку клінічні симптомі можуть бути непомітними, але з ростом дитини деформація прогресує, стає асиметричною та поширюється на ребра, відбуваються необоротні порушення хребта, зростають порушення функції з боку серцево-легеневої системи, формується психологічний комплекс фізичної неповноцінності. У статті розглянуті основні клінічні прояви ВЛДГК, особливості діагностики та визначення показань до вибору методу лікування. Запропоновано алгоритм, оснований на синтезі знань суміжних спеціалістів щодо обсягу необхідних обстежень, сумісної участі мультидисциплінарної команди у встановленні клінічного діагнозу, визначенні найбільш раціональної тактики та виборі сучасних методів лікування у конкретного пацієнта.
Pectus excavatum is the most common congenital chest wall deformity. It creates cosmetic defect, affects the psycho-emotional state and causes functional disorders the organs of mediastinum and lungs. From the beginning, clinical symptoms may not be noticeable, but as a child grows, the deformity progresses, becomes asymmetric and spreads to the ribs, irreversible spine disorders occur, cardiopulmonary system dysfunctions increase, and a psychological complex of physical inferiority is formed. The article discusses the main clinical manifestations of pectus excavatum, diagnostic features, and indications for choosing treatment method. The proposed algorithm is based on the synthesis of the knowledge of related specialists about the scope of necessary examinations, the joint participation of a multidisciplinary team in making a clinical diagnosis, determining the most rational tactics, and choosing modern treatment methods for a specific patient.
вроджена лійкоподібна деформація грудної клітки; обстеження; лікування; діти
pectus excavatum; examination; treatment; children
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Park C.H., Kim T.H., Haam S.J., Lee S. Rib overgrowth may be a contributing factor for pectus excavatum: Evaluation of prepubertal patients younger than 10years old. J. Pediatr. Surg. 2015 Nov. 50(11). 1945-8. doi: 10.1016/j.jpedsurg.2015.07.010.
- Brochhausen C., Turial S., Müller F.K., Schmitt V.H., Coerdt W., Wihlm J.M., et al. Pectus excavatum: history, hypotheses and treatment options. Interact. Cardiovasc. Thorac. Surg. 2012 Jun. 14(6). 801-6. doi: 10.1093/icvts/ivs045.
- Fokin A.A., Steuerwald N.M., Ahrens W.A., Allen K.E. Anatomical, histologic, and genetic characteristics of congenital chest wall deformities. Semin. Thorac. Cardiovasc. Surg. 2009 Spring. 21(1). 44-57. doi: 10.1053/j.semtcvs.2009.03.00.
- Nakaoka T., Uemura S., Yano T., Nakagawa Y., Tanimoto T., Suehiro S. Does overgrowth of costal cartilage cause pectus excavatum? A study on the lengths of ribs and costal cartilages in asymmetric patients. J. Pediatr. Surg. 2009 Jul. 44(7). 1333-6. doi: 10.1016/j.jpedsurg.2008.09.023.
- Haje S.A., Harcke H.T., Bowen J.R. Growth disturbance of the sternum and pectus deformities: imaging studies and clinical correlation. Pediatr. Radiol. 1999. 29. 334-41.
- Chao C.J., Jaroszewski D.E., Kumar P.N., Ewais M.M., Appleton C.P., Mookadam F., et al. Surgical repair of pectus excavatum relieves right heart chamber compression and improves cardiac output in adult patients — an intraoperative transesophageal echocardiographic study. Am. J. Surg. 2015 Dec. 210(6). 1118-24; discussion 1124-5. doi: 10.1016/j.amjsurg.2015.07.006.
- Nuss D., Obermeyer R.J., Kelly R.E. Nuss bar procedure: past, present and future. Ann. Cardiothorac. Surg. 2016 Sep. 5(5). 422-433. doi: 10.21037/acs.2016.08.05.
- Kim S.Y., Jeong J.Y. Pectus excavatum: A rare cause of dysphagia. J. Thorac. Cardiovasc. Surg. 2017 Jan. 153(1). 217. doi: 10.1016/j.jtcvs.2016.04.012.
- Borrhomée S., Lenoir M., Gouton M., Fadel E. Syncope caused by right ventricular obstruction by pectus excavatum. J. Thorac. Cardiovasc. Surg. 2016 Apr. 151(4). e67-9. doi: 10.1016/j.jtcvs.2015.10.018.
- Hsu Y.T., Cheng Y.L., Chang Y.W., Lan C.C., Wu Y.K., Yang M.C. Autonomic nervous system dysregulation in response to postural change in patients with pectus excavatum in Taiwan: a pilot study. J. Cardiothorac. Surg. 2022 May 3. 17(1). 89. doi: 10.1186/s13019-022-01835-5.
- Behr C.A., Denning N.L., Kallis M.P., Maloney C., Soffer S.Z., Romano-Adesman A., et al. The incidence of Marfan syndrome and cardiac anomalies in patients presenting with pectus deformities. J. Pediatr. Surg. 2019 Sep. 54(9). 1926-1928. doi: 10.1016/j.jpedsurg.2018.11.017.
- Kotzot D., Schwabegger A.H. Etiology of chest wall deformities — a genetic review for the treating physician. J. Pediatr. Surg. 2009 Oct. 44(10). 2004-11. doi: 10.1016/j.jpedsurg.2009.07.029.
- Kelly R.E. Jr, Shamberger R.C., Mellins R.B., et al. Prospective multicenter study of surgical correction of pectus excavatum: design, perioperative complications, pain, and baseline pulmonary function facilitated by internet-based data collection. J. Am. Coll. Surg. 2007 Aug. 205(2). 205-216. doi: 10.1016/j.jamcollsurg.2007.03.027.
- Kragten H.A., Siebenga J., Höppener P.F., Verburg R., Visker N. Symptomatic pectus excavatum in seniors (SPES): a cardiovascular problem? A prospective cardiological study of 42 senior patients with a symptomatic pectus excavatum. Neth. Heart J. 2011. 19(2). 73-78. doi: 10.1007/s12471-010-0067-z.
- Koumbourlis A.C. Pectus deformities and their impact on pulmonary physiology. Paediatr. Respir. Rev. 2015. 16(1). 18-24. doi: 10.1016/j.prrv.2014.10.009.
- Billar R.J., Manoubi W., Kant S.G., et al. Association between pectus excavatum and congenital genetic disorders: A systematic review and practical guide for the treating physician. J. Pediatr. Surg. 2021 Dec. 56. 2239-52. doi: 10.1016/j.jpedsurg.2021.04.016.
- Ma I.T., Rebecca A.M., Notrica D.M., McMahon L.E., Jaroszewski D.E. Pectus excavatum in adult women: repair and the impact of prior or concurrent breast augmentation. Plast. Reconstr. Surg. 2015 Feb. 135(2). 303e-312e. doi: 10.1097/PRS.0000000000000990.
- Tanner H., Bischof D., Roten L., et al. Electrocardiographic characteristics of patients with funnel chest before and after surgical correction using pectus bar: a new association with precordial J wave pattern. J. Electrocardiol. 2016 Mar-Apr. 49(2). 174-181. doi: 10.1016/j.jelectrocard.2015.12.004.
- Mocchegiani R., Badano L., Lestuzzi C., Nicolosi G.L., Zanuttini D. Relation of right ventricular morphology and function in pectus excavatum to the severity of the chest wall deformity. Am. J. Cardiol. 1995. 76(12). 941-946.
- Fiorelli S., Capua G., Menna C., et al. Intraoperative cardiac function assessment by transesophageal echocardiography versus FloTrac/Vigileo™ system during pectus excavatum surgical repair. J. Anesth. Analg. Crit. Care. 2021 Dec 9. 1(1). 21. doi: 10.1186/s44158-021-00025-4.
- Lawson M.L., Mellins R.B., Paulson J.F., et al. Increasing severity of pectus excavatum is associated with reduced pulmonary function. J. Pediatr. 2011. 159(2). 256-261.e2. doi: 10.1016/j.jpeds.2011.01.065.
- Gizycka J. Ocena wakazan i metod leczenia operacynjnego lejkowatej bleatki piersiowej u dzici oraz analiza uzyskanych wynikom. Klin. Khirurgii dziecieceg A.M. w. Warszawie, kierownik Panst. Zaki wyd-wo lecarskich. 1962. Vol. 9. P. 480-561.
- Haller J.A. Jr, Kramer S.S., Lietman S.A. Use of CT scans in selection of patients for pectus excavatum surgery: a preliminary report. J. Pediatr. Surg. 1987. 22(10). 904-906.
- Daunt S.W., Cohen J.H., Miller S.F. Age-related normal ranges for the Haller index in children. Pediatr. Radiol. 2004. 34(4). 326-330. doi: 10.1007/s00247-003-1116-1.
- Haecker F.M., Sesia S. Non-surgical treatment of pectus excavatum. J. Vis. Surg. 2016 Mar 23. 2. 63. doi: 10.21037/jovs.2016.03.14.
- Janssen N., Daemen J.H.T., van Polen E.J., Coorens N.A., et al. Pectus Excavatum: Consensus and Controversies in Clinical Practice. Ann. Thorac. Surg. 2023 Jul. 116(1). 191-199. doi: 10.1016/j.athoracsur.2023.02.059.
- Nuss D., Kelly R.E. Jr, Croitoru D.P., Katz M.E. A 10-year review of a minimally invasive technique for the correction of pectus excavatum. J. Pediatr. Surg. 1998 Apr. 33(4). 545-52. doi: 10.1016/s0022-3468(98)90314-1.
- Kelly R.E. Jr, Obermeyer R.J., Goretsky M.J., et al. Recent Modifications of the Nuss Procedure: The Pursuit of Safety During the Minimally Invasive Repair of Pectus Excavatum. Ann. Surg. 2022 Feb 1. 275(2). e496-e502. doi: 10.1097/SLA.0000000000003877.