Резюме
Актуальність. У структурі всіх травматичних ушкоджень хребта переважаючою є зона грудопоперекового переходу, на частку якої припадає понад 53 % всіх переломів хребців. Одним із найбільш клінічно значущих типів ушкоджень у цьому відділі є вибухові переломи. Мета: вивчити напружено-деформований стан моделі грудопоперекового відділу хребта з вибуховим переломом хребця Th12 за різних варіантів транспедикулярної фіксації під впливом стискаючого навантаження. Матеріали та методи. У роботі розроблено та досліджено математичну скінченно-елементну модель грудопоперекового відділу хребта з вибуховим переломом хребця Th12. Вибуховий перелом було модельовано шляхом розділення тіла хребця Th12 на кілька площин, що перетворили його на окремі фрагменти. Проміжки між цими фрагментами заповнювались матеріалом, який імітував міжуламковий регенерат. Розглядались варіанти транспедикулярної стабілізації з використанням різних типів гвинтів, моно- чи бікортикальних, та наявністю чи відсутністю поперечних стяжок. Модель аналізувалась під стискаючим навантаженням. Результати. Максимальний рівень напруження серед кісткових структур, що безпосередньо залучені у фіксацію, було зареєстровано в тілі L2 хребця. Він становив 19,9; 15,6; 19,4 та 15,1 МПа відповідно для моделей з монокортикальними гвинтами без поперечних стяжок, з бікортикальними гвинтами без стяжок, з монокортикальними гвинтами та стяжками, з бікортикальними гвинтами та стяжками. Водночас зона входу гвинта в дугу цього хребця демонструє показники 10,1; 15; 10,2 та 14,3 МПа для цих моделей відповідно. Пікові навантаження на елементи металоконструкції спостерігаються на опорних балках і становлять 212,5; 159,6; 203,7; 142,8 МПа відповідно для розглянутих моделей. Висновки. Результати дослідження показали, що під впливом стискаючого навантаження при моделюванні вибухового перелому ділянки грудопоперекового переходу використання довгих гвинтів призводить до зниження рівня напружень як в елементах металевої конструкції, так і в кісткових елементах моделі, тоді як застосування поперечних стяжок має незначний вплив.
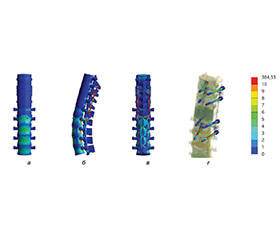
Background. In the structure of all traumatic spine injuries, the thoracolumbar junction is predominant, accounting for over 53 % of all vertebral fractures. One of the most clinically significant types of injuries in this area are burst fractures. The purpose was to study the stress-strain state of the thoracolumbar spine model with a burst fracture of the Th12 vertebra in various transpedicular fixation options under compression load. Materials and methods. The study developed and investigated a finite element model of the thoracolumbar spine with a burst fracture of the Th12 vertebra. The burst fracture was modeled by dividing the vertebral body of the Th12 into several planes, transforming it into separate fragments. The gaps between these fragments were filled with a material that simulated the interfragmentary regenerate. Variants of transpedicular stabilization using different types of screws, mono- or bicortical, and with or without cross-links, were examined. The model was analyzed under compression load. Results. The maximum level of stress among the bone structures directly involved in fixation was registered in the L2 vertebral body. It amounted to 19.9, 15.6, 19.4, and 15.1 MPa, respectively, for models with monocortical screws without cross-links, bicortical screws without cross-links, monocortical screws with cross-links, bicortical screws with cross-links. Simultaneously, the zone of screw entry into the arch of this vertebra shows values of 10.1, 15, 10.2, and 14.3 MPa for these models, respectively. Peak loads on the metal structure elements are observed on the rods, amounting to 212.5, 159.6, 203.7, 142.8 MPa, respectively, for the considered models. Conclusions. The results of the study showed that under the influence of compression load when modeling a burst fracture of the thoracolumbar junction, the use of long screws leads to a reduction in stress levels, both in the elements of the metal structure and in the bone elements of the model, while the use of cross-links has a negligible effect.
Список литературы
1. Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet. 2020;396(10258):1204-1222. doi: 10.1016/S0140-6736(20)30925-9.
2. Nekhlopochyn OS, Nikiforova AN, Verbov VV, Yovenko TA, Cheshuk IV. Analysis of the Epidemiology of Traumatic Vertebral Column Injuries in Eastern European Countries. Ukrainian Neurosurgical Journal. 2023;29(4):22-34. doi: 10.25305/unj.286922.
3. Baaj AA, Downes K, Vaccaro AR, Uribe JS, Vale FL. Trends in the treatment of lumbar spine fractures in the United States: a socioeconomics perspective: clinical article. J Neurosurg Spine. 2011;15(4):367-370. doi: 10.3171/2011.5.Spine10934, PMID: 21740124.
4. Bouyer B, Vassal M, Zairi F, Dhenin A, Grelat M, Dubory A, et al. Surgery in vertebral fracture: epidemiology and functional and radiological results in a prospective series of 518 patients at 1 year’s follow-up. Orthopaedics & traumatology, surgery & research: OTSR. 2015;101(1):11-15. doi: 10.1016/j.otsr.2014.11.012, PMID: 25596983.
5. Liu P, Yao Y, Liu MY, Fan WL, Chao R, Wang ZG, et al. Spinal trauma in mainland China from 2001 to 2007: an epidemiological study based on a nationwide database. Spine (Phila Pa 1976). 2012;37(15):1310-1315. doi: 10.1097/BRS.0b013e3182474d8b, PMID: 22744399.
6. Wang H, Zhang Y, Xiang Q, Wang X, Li C, Xiong H, et al. Epidemiology of traumatic spinal fractures: experience from medical university-affiliated hospitals in Chongqing, China, 2001-2010. J Neurosurg Spine. 2012;17(5):459-468. doi: 10.3171/2012.8.Spine111003, PMID: 22978439.
7. Dai LY, Jiang SD, Wang XY, Jiang LS. A review of the management of thoracolumbar burst fractures. Surg Neurol. 2007;67(3):221-231; discussion 231. doi: 10.1016/j.surneu.2006.08.081, PMID: 17320622.
8. Vaccaro AR, Oner C, Kepler CK, Dvorak M, Schnake K, Bellabarba C, et al. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine (Phila Pa 1976). 2013;38(23):2028-2037. doi: 10.1097/BRS.0b013e3182a8a381, PMID: 23970107.
9. Woo JH, Lee HW, Choi HJ, Kwon YM. Are "Unstable" Burst Fractures Really Unstable? J Korean Neurosurg Soc. 2021;64(6):944-949. doi: 10.3340/jkns.2021.0080, PMID: 34689477.
10. Verheyden AP, Spiegl UJ, Ekkerlein H, Gercek E, Hauck S, Josten C, et al. Treatment of Fractures of the Thoracolumbar Spine: Recommendations of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU). Global Spine J. 2018;8(2 Suppl):34s-45s. doi: 10.1177/2192568218771668, PMID: 30210959.
11. Sharif S, Shaikh Y, Yaman O, Zileli M. Surgical Techniques for Thoracolumbar Spine Fractures: WFNS Spine Committee Recommendations. Neurospine. 2021;18(4):667-680. doi: 10.14245/ns.2142206.253, PMID: 35000320.
12. Weiser TG, Haynes AB, Molina G, Lipsitz SR, Esquivel MM, Uribe-Leitz T, et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet (London, England). 2015;385 Suppl 2:S11. doi: 10.1016/S0140-6736(15)60806-6, PMID: 26313057.
13. Tan T, Huang MS, Rutges J, Marion TE, Fitzgerald M, Hunn MK, et al. Rate and Predictors of Failure in the Conservative Management of Stable Thoracolumbar Burst Fractures: A Systematic Review and Meta-Analysis. Global Spine J. 2022;12(6):1254-1266. doi: 10.1177/21925682211031207, PMID: 34275348.
14. Sharif S, Zileli M. Introduction to Thoracolumbar Spine Fractures: WFNS Spine Committee Recommendations. Neurospine. 2021;18(4):651-653. doi: 10.14245/ns.2143240.620, PMID: 35000317.
15. Calleros-Hernández NA, Valencia-Martínez G, Hardy-Pérez AE, Granados-Agonizante I. [Percutaneous versus open technique transpedicular fixation in patients with thoracolumbares type A fractures]. Acta Ortop Mex. 2019;33(4):217-224. PMID: 32246591.
16. Nekhlopochyn O, Verbov V, Cheshuk I, Karpinsky M, Yaresko O. Mathematical Modeling of Variants of Transpedicular Fixation at the Thoracolumbar Junction after ТhХІІ Vertebrectomy during Trunk Backward Bending. Orthopaedics Traumatology аnd Prosthetics. 2023(2):43-49. doi: 10.15674/0030-59872023243-49.
17. Nekhlopochyn OS, Verbov VV, Cheshuk IV, Karpinsky MY, Yaresko OV. Finite Element Analysis of Thoracolumbar Junction Transpedicular Fixation Variants after Resection of the Th12 Vertebra While Forward Bending. Bulletin of Problems Biology and Medicine. 2023;169(2):281-287. doi: 10.29254/2077-4214-2023-2-169-281-296.
18. Cowin SC. Bone Mechanics Handbook. 2nd ed. Boca Raton: CRC Press; 2001.
19. Boccaccio A, Pappalettere C. Mechanobiology of Fracture Healing: Basic Principles and Applications in Orthodontics and Orthopaedics. In: Klika V, editor. Theoretical Biomecha-nics. Croatia: InTech; 2011. Р. 21-48.
20. Nekhlopochin A, Nekhlopochin S, Karpinsky M, Shvets A, Karpinskaya E, Yaresko A. Mathematical Ana-lysis and Optimization of Design Characteristics of Stabilizing Vertebral Body Replacing Systems for Subaxial Cervical Fusion Using the Finite Element Method. Hirurgiâ Рozvonočnika. 2017;14(1):37-45. doi: 10.14531/ss2017.1.37-45.
21. Radchenko VA, Kutsenko VA, Popov AI, Karpinskуi MY, Karpinska OD. Modeling the variants of transpedicular fixation of the thoracic spine in the rejection of one-three vertebrae. Trauma. 2022;18(5):95-102. doi: 10.22141/1608-1706.5.18.2017.114125.
22. Niinomi M. Mechanical biocompatibilities of titanium alloys for biomedical applications. J Mech Behav Biomed Mater. 2008;1(1):30-42. doi: 10.1016/j.jmbbm.2007.07.001, PMID: 19627769.
23. Зенкевич О.К. Метод конечных элементов в технике. Москва: Мир, 1975. 271 с.
24. Алямовский А. COSMOSWorks. Основы расчета конструкций в среде SolidWorks: ЛитРес, 2022.
25. Lynn G, Mukherjee DP, Kruse RN, Sadasivan KK, Albright JA. Mechanical stability of thoracolumbar pedi-cle screw fixation. The effect of crosslinks. Spine (Phila Pa 1976). 1997;22(14):1568-1572; discussion 1573. doi: 10.1097/00007632-199707150-00007, PMID: 9253090.
26. Cornaz F, Widmer J, Snedeker JG, Spirig JM, Farshad M. Cross-links in posterior pedicle screw-rod instrumentation of the spine: a systematic review on mechanical, biomechanical, numerical and clinical studies. Eur Spine J. 2021;30(1):34-49. doi: 10.1007/s00586-020-06597-z, PMID: 33009949.
27. Bruno AG, Burkhart K, Allaire B, Anderson DE, Bouxsein ML. Spinal Loading Patterns From Biomechanical Modeling Explain the High Incidence of Vertebral Fractures in the Thoracolumbar Region. Journal of Bone аnd Mineral Research: the official journal of the American Society for Bone and Mineral Research. 2017;32(6):1282-1290. doi: 10.1002/jbmr.3113, PMID: 28244135.