
Журнал «Боль. Суставы. Позвоночник» Том 14, №1, 2024
Вернуться к номеру
Оцінка м’язової маси та функції у хворих на ревматоїдний артрит
Авторы: Стойка І.В., Яцишин Р.І., Дрогомерецька О.І., Попадинець І.Р., Бабенко О.І., Шаповал О.А.
Івано-Франківський національний медичний університет, м. Івано-Франківськ, Україна
Рубрики: Ревматология, Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
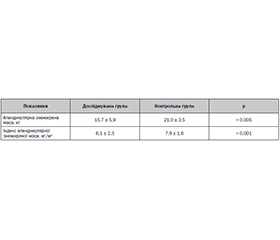
Актуальність. Саркопенія у хворих на ревматоїдний артрит (РА) виникає у зв’язку з хронічним запальним процесом, гормональною терапією та обмеженням фізичної активності через больовий синдром. Для пацієнтів з РА важливо зберігати м’язову масу та функцію, щоб зменшити ризик інвалідності та поліпшити якість життя. Метою роботи була оцінка м’язової маси та функції у хворих на РА з порівнянням методів визначення маси скелетних м’язів, рекомендованих EWCSOP2. Матеріали та методи. Усього обстежено 44 особи, з яких 32 хворі на РА та 12 практично здорових осіб контрольної групи. У дослідженні використані наступні методи: опитувальник SARC-F, визначення апендикулярної маси скелетних м’язів за допомогою двофотонної рентгенівської абсорбціометрії (ДРА), відсотків м’язової та жирової тканини за допомогою біоімпедансометрії, визначення площі поперечного перерізу поперекового м’яза за допомогою комп’ютерної томографії (КТ), тести на фізичну працездатність. Пацієнтів з РА було розділено на 3 групи: група А (11 осіб) — проведено анкетування (SARC-F), оцінку сили скелетних м’язів та визначення маси м’язів за допомогою ДРА; група В (11 пацієнтів) — опитування (SARC-F), оцінку сили скелетних м’язів та визначення маси м’язів за допомогою біоімпедансометрії; група С (10 пацієнтів) — анкетування (SARC-F), оцінку сили скелетних м’язів і визначення маси м’язів за допомогою КТ. Результати. Усі показники функціональних тестів та методів оцінки м’язової маси були вірогідно гіршими у хворих на РА порівняно з контрольною групою. У 50 % хворих на РА діагностована саркопенія, 6 випадків у групі А (середнє значення апендикулярної знежиреної маси становило у них 15,7 кг, у контрольній групі — 21 кг), 5 у групі В (середні показники частки м’язової маси становили 21,2 % порівняно з 29,3 % у групі контролю) та 5 у групі С (середні показники частки м’язової маси становили 49,46 %, у групі контролю — 58,32 %). Висновки. Кожен з методів оцінки маси скелетних м’язів довів свою спроможність в діагностиці саркопенії. Підвищення ефективності діагностики саркопенії у хворих на РА дозволить як удосконалити відповідь на лікування основного захворювання, так і поліпшити якість життя пацієнтів.
Background. Sarcopenia in patients with rheumatoid arthritis (RA) occurs in connection with the chronic inflammatory process, hormonal therapy, and limitation of physical activity due to pain syndrome. For RA patients, it is important to preserve muscle mass and function to reduce the risk of disability and improve quality of life. The research purposed to assess muscle mass and function in RA patients with a comparison of methods for determining skeletal muscle mass recommended by EWCSOP2. Materials and methods. A total of 44 persons were examined, 32 were patients with RA, and 12 ones were healthy persons (the control group). The following methods were used in the study: the SARC-F questionnaire, the determination of the appendicular mass of skeletal muscles using dual-photon X-ray absorptiometry (DXA), the percentage of muscle and fat tissue using bioimpedancemetry, the determination of the cross-sectional area of the lumbar muscle using computer tomography (CT), physical performance tests. Patients with RA were divided into 3 groups: group A (11 persons) — questionnaire (SARC-F), assessment of skeletal muscle strength and determination of muscle mass using DXA was performed; group B (11 patients) — questionnaire (SARC-F), assessment of skeletal muscle strength and determination of muscle mass using bioimpedancemetry; group C (10 persons) — questionnaire (SARC-F), assessment of skeletal muscle strength and determination of muscle mass using CT. Results. All indices of physical performance tests and instrumental methods of assessing muscle mass were significantly worse in patients with RA compared to the control group. Sarcopenia was diagnosed in 50 % of patients with RA, 6 cases in group A (the average value of appendicular lean mass was 15.7 kg in them, in the control group — 21 kg), 5 in group B (the average values of the proportion of muscle mass were 21.2 compared to 29.3 % in the control group) and 5 in group C (the average percentage of muscle mass was 49.46 %, in the control group 58.32 %). Conclusions. Each of the methods of assessing the mass of skeletal muscles has proven its ability in the diagnosis of sarcopenia. Improving the efficiency of diagnosing sarcopenia in patients with RA will improve the response to the treatment of the underlying disease and improve the quality of life of patients.
ревматоїдний артрит; м’язова сила; м’язова маса; саркопенія; біоімпедансометрія; двофотонна рентгенівська абсорбціометрія; комп’ютерна томографія
rheumatoid arthritis; muscle strength; muscle mass; sarcopenia; bioimpedancemetry; two-photon X-ray absorptiometry; computed tomography
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Dzerovych N. Європейські рекомендації 2019 року щодо діагностики саркопенії. Біль. Суглоби. Хребет. 2019. 9(4). 257-261. doi: 10.22141/2224-1507.9.4.2019.191925.
- Cruz-Jentoft A.J., Bahat G., Bauer J., Boirie Y., Bruyère O., Cederholm T., et al.; Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019 Jan 1. 48(1). 16-31. doi: 10.1093/ageing/afy169. Erratum in: Age Ageing. 2019 Jul 1. 48(4). 601. PMID: 30312372; PMCID: PMC6322506.
- Pascual-Fernández J., Fernández-Montero A., Córdova-Martínez A., Pastor D., Martínez-Rodríguez A., Roche E. Sarcopenia: Molecular Pathways and Potential Targets for Intervention. Int. J. Mol. Sci. 2020 Nov 22. 21(22). 8844. doi: 10.3390/ijms21228844. PMID: 33266508; PMCID: PMC7700275.
- Schaap L.A., van Schoor N.M., Lips P., Visser M. Associations of Sarcopenia Definitions, and Their Components, With the Incidence of Recurrent Falling and Fractures: The Longitudinal Aging Study Amsterdam. J. Gerontol. A Biol. Sci. Med. Sci. 2018 Aug 10. 73(9). 1199-1204. doi: 10.1093/gerona/glx245. PMID: 29300839.
- Povoroznyuk V.V., Dzerovych N.I., Ivanyk O.S., Karasevska T.A. Sarcopenia and Rheumatoid Arthritis. Pain, Joints, Spine. 2019. 9(2). 83-89. doi: 10.22141/2224-1507.9.2.2019.172120.
- Povoroznyuk V., Binkley N., Dzerovych N., Povoroznyuk R. Sarkopeniya [Sarcopenia]. Kyiv, 2016. 180 p. (in Ukrainian).
- Krajewska-Włodarczyk M. [Sarcopenia in rheumatoid arthritis]. Wiad Lek. 2016. 69(3 pt 2). 542-547. Polish. PMID: 27717942.
- Doğan S.C., Hizmetli S., Hayta E., Kaptanoğlu E., Erselcan T., Güler E. Sarcopenia in women with rheumatoid arthritis. Eur. J. Rheumatol. 2015 Jun. 2(2). 57-61. doi: 10.5152/eurjrheum.2015.0038. Epub 2015 Mar 31. PMID: 27708927; PMCID: PMC5047263.
- Moschou D., Krikelis M., Georgakopoulos C., Mole E., Chronopoulos E., Tournis S., et al. Sarcopenia in Rheumatoid arthritis. A narrative review. J. Frailty Sarcopenia Falls. 2023 Mar 1. 8(1). 44-52. doi: 10.22540/JFSF-08-044. PMID: 36873824; PMCID: PMC9975974.
- Dzhus M.B., Kulyk M.S., Karasevska T.A. et al. Sarcopenia and Rheumatic Diseases: Is There Any Connection. Pain, Joints, Spine. 2022. 12(4). 201-210. doi: 10.22141/pjs.12.4.2022.349.
- Cawthon P.M. Assessment of Lean Mass and Physical Performance in Sarcopenia. J. Clin. Densitom. 2015 Oct-Dec. 18(4). 467-71. doi: 10.1016/j.jocd.2015.05.063. Epub 2015 Jun 10. PMID: 26071168.
- Welch S.A., Ward R.E., Beauchamp M.K., Leveille S.G., Travison T., Bean J.F. The Short Physical Performance Battery (SPPB): A Quick and Useful Tool for Fall Risk Stratification Among Older Primary Care Patients. J. Am. Med. Dir. Assoc. 2021 Aug. 22(8). 1646-1651. doi: 10.1016/j.jamda.2020.09.038. Epub 2020 Nov 13. PMID: 33191134; PMCID: PMC8113335.
- Carvalho G.D., Bonfiglioli K., Caparbo V.F., Takayama L., Pereira R.M.R., Domiciano D.S. Changes to Body Composition in Women with Long-Standing Established Rheumatoid Arthritis: Differences by Level of Disease Activity. J. Clin. Densitom. 2020 Oct-Dec. 23(4). 639-646. doi: 10.1016/j.jocd.2019.06.002. Epub 2019 Jun 13. PMID: 31285112.
- Gonzalez M.C., Heymsfield S.B. Bioelectrical impedance analysis for diagnosing sarcopenia and cachexia: what are we really estimating? J. Cachexia Sarcopenia Muscle. 2017 Apr. 8(2). 187-189. doi: 10.1002/jcsm.12159. Epub 2017 Jan 31. PMID: 28145079; PMCID: PMC5377383.
- Gonzalez M.C., Barbosa-Silva T.G., Heymsfield S.B. Bioelectrical impedance analysis in the assessment of sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care. 2018 Sep. 21(5). 366-374. doi: 10.1097/MCO.0000000000000496. PMID: 29957677.
- Lortie J., Gage G., Rush B., Heymsfield S.B., Szczykutowicz T.P., Kuchnia A.J. The effect of computed tomography parameters on sarcopenia and myosteatosis assessment: a scoping review. J. Cachexia Sarcopenia Muscle. 2022 Dec. 13(6). 2807-2819. doi: 10.1002/jcsm.13068. Epub 2022 Sep 5. PMID: 36065509; PMCID: PMC9745495.
- Dodds R.M., Syddall H.E., Cooper R., Benzeval M., Deary I.J., Dennison E.M., et al. Grip strength across the life course: normative data from twelve Bri–tish studies. PLoS One. 2014 Dec 4. 9(12). e113637. doi: 10.1371/journal.pone.0113637. PMID: 25474696; –PMCID: PMC4256164.
- Batsis J.A., Mackenzie T.A., Barre L.K., Lopez-Jimenez F., Bartels S.J. Sarcopenia, sarcopenic obesity and mortality in older adults: results from the National Health and Nutrition Examination Survey III. Eur. J. Clin. Nutr. 2014 Sep. 68(9). 1001-7. doi: 10.1038/ejcn.2014.117. Epub 2014 Jun 25. PMID: 24961545.
- Bennett J.L., Pratt A.G., Dodds R., Sayer A.A., Isaacs J.D. Rheumatoid sarcopenia: loss of skeletal muscle strength and mass in rheumatoid arthritis. Nat. Rev. Rheumatol. 2023 Apr. 19(4). 239-251. doi: 10.1038/s41584-023-00921-9. Epub 2023 Feb 17. PMID: 36801919.
- An H.J., Tizaoui K., Terrazzino S., Cargnin S., Lee K.H., Nam S.W., et al. Sarcopenia in Autoimmune and Rheumatic Diseases: A Comprehensive Review. Int. J. Mol. Sci. 2020 Aug 7. 21(16). 5678. doi: 10.3390/ijms21165678. PMID: 32784808; PMCID: PMC7461030.
- Tada M., Yamada Y., Mandai K., Hidaka N. Matrix metalloprotease 3 is associated with sarcopenia in rheumatoid arthritis — results from the CHIKARA study. Int. J. Rheum. Dis. 2018 Nov. 21(11). 1962-1969. doi: 10.1111/1756-185X.13335. Epub 2018 Sep 5. PMID: 30187662.
- Reina D., Gómez-Vaquero C., Díaz-Torné C., Solé J.M.N.; Rheumatology Service. Hospital Moisès Broggi. Assessment of nutritional status by dual X-Ray absorptiometry in women with rheumatoid arthritis: A case-control study. Medicine (Baltimore). 2019 Feb. 98(6). e14361. doi: 10.1097/MD.0000000000014361. PMID: 30732168; PMCID: PMC6380876.
- Tada M., Yamada Y., Mandai K., Hidaka N. Screening for sarcopenia and obesity by measuring thigh muscle and fat thickness by ultrasound in patients with rheumatoid arthritis. Osteoporos Sarcopenia. 2021 Jun. 7(2). 81-87. doi: 10.1016/j.afos.2021.06.002. Epub 2021 Jun 16. PMID: 34278004; PMCID: PMC8261725.
- Torii M., Hashimoto M., Hanai A., Fujii T., Furu M., Ito H., et al. Prevalence and factors associated with sarcopenia in patients with rheumatoid arthritis. Mod. Rheumatol. 2019 Jul. 29(4). 589-595. doi: 10.1080/14397595.2018.1510565. Epub 2018 Sep 11. PMID: 30092163.
- Yatsyshyn R., Stoika І. Phenotypes of secondary sarcopenia in patients with rheumatoid arthritis. Annals of the Rheumatic Diseases. 2018. 77. 1351. doi: 10.1136/annrheumdis-2018-eular.2305.