
Журнал «Медицина неотложных состояний» Том 20, №3, 2024
Вернуться к номеру
Зміни показників гемодинаміки та транспорту кисню у хворих з ідіопатичною легеневою артеріальною гіпертензією залежно від їх виживання
Авторы: Боцюк Ю.А., Сіренко Ю.М.
Національний університет охорони здоров’я України імені П.Л. Шупика, м. Київ, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
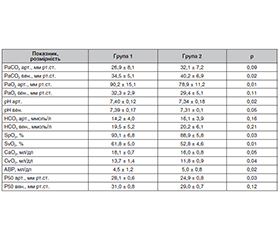
Актуальність. Ідіопатична легенева артеріальна гіпертензія (ІЛАГ) — тяжке захворювання, що вражає судини малого кола кровообігу та призводить до правошлуночкової недостатності і смерті пацієнтів. Показники гемодинаміки та транспорту кисню відіграють центральну роль у прогресуванні та розвитку захворювання. Мета: визначити показники гемодинаміки, транспорту кисню. Матеріали та методи. У дослідження включено 124 хворі з ІЛАГ. Проведено розподіл пацієнтів на дві групи: живі пацієнти (група 1) та ті, що померли (група 2). Усім пацієнтам проведено загальноклінічні дослідження, тест із 6-хвилинною ходьбою, трансторакальну та спекл-трекінг ехокардіографію, катетеризацію правих відділів серця, визначення газового складу крові та обрахунок показників гемодинаміки. Результати. Ми обчислили та порівняли в обох групах хворих індекс ударної роботи правого (ІУРПШ) (19,93 ± 7,84 проти 16,47 ± 4,67 г·м·м–2, р = 0,009) та лівого шлуночка (ІУРЛШ) (39,47 ± 10,53 проти 35,92 ± 11,19 г·м·м–2, р = 0,036) та їх співвідношення (ІУРПШ/ІУРЛШ) (0,59 ± 0,16 проти 0,46 ± 0,13, р = 0,008), насосний коефіцієнт правого та лівого шлуночка (НКПШ, НКЛШ) (97 ± 2,16 проти 1,82 ± 1,04 г·м, р = 0,001; та 5,36 ± 4,84 проти 4,41 ± 2,15 г·м, р = 0,04 відповідно) та їх співвідношення (НКПШ/НКЛШ) (0,54 ± 0,19 проти 0,44 ± 0,11, р = 0,05). Також ми знайшли відмінності у показниках парціального тиску СО2 (PaCO2) венозної крові (34,5 ± 5,1 проти 40,2 ± 6,9 мм рт.ст., p = 0,02), парціального тиску О2 (PaO2) артеріальної крові (90,2 ± 15,1 проти 78,9 ± 11,2 мм рт.ст., p = 0,01), артеріально-венозної різниці (АВР) вмісту кисню (4,5 ± 1,2 проти 5,0 ± 0,8 мл/дл, p = 0,02) між обома групами. Висновки. ІУРПШ, ІУРЛШ, ІУРПШ/ІУРЛШ, НКПШ, НКЛШ, НКПШ/НКЛШ вірогідно відрізнялися між групами. Використання вищенаведених показників гемодинаміки може допомогти у більш глибокому розумінні прогнозу у цієї категорії хворих. Визначення показників транспорту кисню (PaCO2, PaO2) та АВР у хворих з ІЛАГ забезпечує краще розуміння статусу та прогнозу захворювання у цієї групи пацієнтів.
Background. Idiopathic pulmonary arterial hypertension (IPAH) is a severe disease that affects the vessels of the pulmonary circulation and leads to right ventricular failure and death of patients. Indicators of hemodynamics and oxygen transport play central role in the progression and development of the disease. Objective: to evaluate indicators of hemodynamics, oxygen transport. Materials and methods. The study included 124 patients with IPAH. They were divided into two groups: alive patients (group 1) and those who died (group 2). All of them underwent general clinical examinations, a 6-minute walk test, transthoracic and speckle tracking echocardiography, right heart catheterization, blood gas analysis and calculation of hemodynamic parameters. Results. We calculated and compared the right (RVSWI) (19.93 ± 7.84 vs. 16.47 ± 4.67 g·m·m–2, p = 0.009) and left ventricular stroke work index (LVSWI) (39.47 ± 10.53 vs. 35.92 ± 11.19 g·m·m–2, p = 0.036) and their ratio (RVSWI/LVSWI) (0.59 ± 0.16 vs. 0.46 ± ± 0.13, p = 0.008), right (RVPC) (97.00 ± 2.16 vs. 1.82 ± 1.04 g·m, p = 0.001) and left ventricular pump coefficient (LVPC) (5.36 ± 4.84 vs. 4.41 ± 2.15 g·m, p = 0.04) and their ratio (RVPC/LVPC) (0.54 ±0.19 vs. 0.44 ± 0.11, p = 0.05) in both groups of patients. Also, we found differences in partial pressure of carbon dioxide (PaCO2) of venous blood (34.5 ± 5.1 vs. 40.2 ± 6.9 mm Hg, p = 0.02), partial pressure of oxygen (PaO2) of arterial blood (90.2 ± 15.1 vs. 78.9 ± 11.2 mm Hg; p = 0.01), arteriovenous oxygen difference (A-vO2) (4.5 ± 1.2 vs. 5.0 ± 0.8 ml/dL, p = 0.02) between both groups. Conclusions. RVSWI, LVSWI, RVSWI/LVSWI, RVPC, LVPC, RVPC/LVPC were significantly different between the groups. The use of the above hemodynamic parameters can help in a deeper understanding of the prognosis in IPAH patients. Performance of oxygen transport indicators (PaCO2, PaO2) and A-vO2 in IPAH patients provides a broader understanding of the status and prognosis of this disease.
легенева гіпертензія; гемодинаміка; газовий склад крові
pulmonary hypertension; hemodynamics; blood gas analysis
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Humbert M, Kovacs G, Hoeper M, Badagliacca R, Berger R et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: Developed by the task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Endorsed by the International Society for Heart and Lung Transplantation (ISHLT) and the European Reference Network on rare respiratory diseases (ERN-LUNG). European Heart Journal. 2022 Oct 7;43, Iss. 38:3618-3731.
- Zanatta E, Polito P, Famoso G, Larosa M, De Zorzi E et al. Pulmonary arterial hypertension in connective tissue disorders: Pathophysiology and treatment. Exp Biol Med (Maywood). 2019 Feb;244(2):120-131.
- Hsu S, Houston BA, Tampakakis E, Bacher AC, Rhodes PS et al. Right ventricular functional reserve in pulmonary arterial hypertension. Circulation. 2016;133:2413-22. doi: 10.1161/CIRCULATIONAHA.116.022082.
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002 Jul 1;166(1):111-7. doi: 10.1164/ajrccm.166.1.at1102.
- Mazimba S, Welch TS, Mwansa H, Breathett KK, Kennedy JLW et al. Haemodynamically derived pulmonary artery pulsatility index predicts mortality in pulmonary arterial hypertension. Heart Lung Circ. 2019;28:752-760.
- Prieto O, Cianciulli TF, Stewart-Harris A, Rodriguez A, Saccheri MC et al. Speckle Tracking Imaging in Patients with Pulmonary Hypertension. J Cardiovasc Imaging. 2021 Jul;29(3):236-251. doi: 10.4250/jcvi.2020.0192.
- Voigt JU, Pedrizzetti G, Lysyansky P, Marwick TH, Houle H et al. Definition for a common standard for 2D speckle-tracking echpcardiography: consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur Heart J Cardiovasc Imaging. 2015 Jan;16(1):1-11. Doi: 10-1093/ehjci/jeu184. Epub 2014 Dec 18. PMID: 25525063.
- Сіренко Ю.М., Живило І.О., Радченко Г.Д., Боцюк Ю.А. Діагностичне значення катетеризації правих відділів серця та легеневої артерії у хворих з підозрою на легеневу гіпертензію. Частина 2. Інвазивне дослідження показників гемодинаміки та транспорту кисню. Український кардіологічний журнал. 2021. Т. 28. № 4. С. 9-22.
- Ekeloef NP, Ekirsen J, Kancir CB. Evaluation of two methods to calculate p50 from a single blood sample. Anaesthesiologica Scandinavica. 2001;45(5):550-552. doi: 10.1034/j.1399-6576.2001.045005550.x.
- Siggaard-Andersen O., Siggaard-Andersen M. The Oxygen Status Algorithm. A computer program for calculation and displaying pH and blood gas data. Scand. J. Clin. Lab. Invest. 1990;50(203):29-45. doi: 10.3109/00365519009087489.
- Liu BY, Wu WC, Zeng QX, Liu ZH, Niu LL et al. Comparison of the capability of risk strati-fication evaluation between two- and three-dimensional speckle-tracking strain in pre-capillary pulmonary hypertension. Pulm Circ. 2019 Dec 27;9(4):2045894019894525. doi: 10.1177/2045894019894525. PMID: 31908764; PMCID: PMC6935885.
- Mahran Y, Schueler R, Weber M, Pizarro C, Nickenig G et al. Noninvasive model including right ventricular speckle tracking for the evaluation of pulmonary hypertension. World J Cardiol. 2016 Aug 26;8(8):472-80. doi: 10.4330/wjc.v8.i8.472. PMID: 27621775; PMCID: PMC4997528.
- Cianciulli TF, Prieto O, Stewart-Harris A, Rodríguez AS, Saccheri MC, Gagliardi JA. Subcos-tal right ventricular free wall strain in patients with pulmonary hypertension. Medicina (B Aires). 2023;83(1):19-28. English. PMID: 36774593.
- Badano LP, Kolias TJ, Muraru D. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: a consensus docu-ment of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur Heart J Cardiovasc Imaging. 2018;19:591-600.
- Kato T, Kasai T, Suda S, Sato A, Ishiwata S et al. Prognostic effects of arterial carbon dioxide levels in patients hospitalized into the cardiac intensive care unit for acute heart failure. Eur Heart J Acute Cardiovasc Care. 2021 Jun 30;10(5):497-502. doi: 10.1093/ehjacc/zuab001. PMID: 34192746; PMCID: PMC8245141.
- Aetou M, Wahab L, Dreher M, Daher A. Significance of Hypocapnia in the Risk Assessment of Patients with Pulmonary Hypertension. J Clin Med. 2023 Sep 30;12(19):6307. doi: 10.3390/jcm12196307. PMID: 37834951; PMCID: PMC10573368.
- Hoeper MM, Pletz MW, Golpon H, Welte T. Prognostic value of blood gas analyses in patients with idiopathic pulmonary arterial hypertension. Eur Respir J. 2007 May;29(5):944-50. doi: 10.1183/09031936.00134506. Epub 2007 Feb 14. PMID: 17301100.
- Nazzareno Galiè, Vallerie V. McLaughlin, Lewis J. Rubin, Gerald Simonneau. European Respiratory Journal. 2019;53:1802148. DOI: 10.1183/13993003.02148-2018.
- Maurer SJ, Habdank V, Hörer J, Ewert P, Tutarel O. NT-proBNP Is a Predictor of Mortality in Adults with Pulmonary Arterial Hypertension Associated with Congenital Heart Disease. J Clin Med. 2023 Apr 24;12(9):3101. doi: 10.3390/jcm12093101. PMID: 37176542; PMCID: PMC10179459.
- Suntharalingam J, Goldsmith K, Toshner M, Doughty N, Sheares KK et al. Role of NT-proBNP and 6MWD in chro-nic thromboembolic pulmonary hypertension. Respir Med. 2007 Nov;101(11):2254-62. doi: 10.1016/j.rmed.2007.06.027. Epub 2007 Aug 13. PMID: 17706409.
- Raitière O, Berthelot E, Fauvel C, Guignant P, Si Belkacem N, Sitbon O, Bauer F. The dan-gerous and contradictory prognostic significance of PVR<3WU when TAPSE<16mm in postcapillary pul-monary hypertension. ESC Heart Fail. 2020 Oct;7(5):2398-2405. doi: 10.1002/ehf2.12785. Epub 2020 Jul 23. PMID: 32705818; PMCID: PMC7524100.
- Mazurek JA, Vaidya A, Mathai SC, Roberts JD, Forfia PR. Follow-up tricuspid annular plane systolic excursion predicts survival in pulmonary arterial hypertension. Pulm Circ. 2017 Apr-Jun;7(2):361-371. doi: 10.1177/2045893217694175. Epub 2017 Mar 13. PMID: 28597759; PMCID: PMC5467921.
- Li Y, Wang T, Haines P, Li M, Wu W, Liu M, et al. Prognostic value of right ventricular two-dimensional and three-dimensional speckle-tracking strain in pulmonary arterial hypertension: Superiority of longitudinal strain over circumferential and radial strain. J Am Soc Echocardiogr. 2020;33:985-994.e1. doi: 10.1016/j.echo.2020.03.015.
- Kind T, Mauritz GJ, Marcus JT, van de Veerdonk M, Westerhof N, Vonk-Noordegraaf A. Right ventricular ejection fraction is better reflected by transverse rather than longitudinal wall motion in pulmonary hypertension. J Cardiovasc Magn Reson. 2010;12:35. doi: 10.1186/1532-429x-12-35.
- Li Q, Zhang Y, Cui X, Lu W, Ji Q, Zhang M. Optimal combination of right ventricular functional parameters using echocardio-graphy in pulmonary arterial hypertension. ESC Heart Failure. 2024. https://doi.org/10.1002/ehf2.14752.
- Armstrong HF, Schulze PC, Kato TS, Bacchetta M, Thirapatarapong W, Bartels MN. Right ventricular stroke work index as a negative predictor of mortality and initial hospital stay after lung transplantation. J Heart Lung Transplant. 2013;32:603-8. doi: 10.1016/j.healun.2013.03.004.
- Matthews JC, Koelling TM, Pagani FD, Aaronson KD. The right ventricular failure risk score a pre-operative tool for assessing the risk of right ventricular failure in left ventricular assist device candidates. J Am Coll Cardiol. 2008;51:2163-72. doi: 10.1016/j.jacc.2008.03.009.
- Bilchick KC, Mejia-Lopez E, McCullough P, Breathett K, Kennedy JL, Tallaj J et al. Clinical Impact of Changes in Hemodynamic Indices of Contractile Function During Treatment of Acute Decompen-sated Heart Failure. J Card Fail. 2018 Jan;24(1):43-50. doi: 10.1016/j.cardfail.2017.07.001. Epub 2017 Jul 13. PMID: 28712955.