
Международный эндокринологический журнал Том 20, №3, 2024
Вернуться к номеру
Удосконалення терапії ішемічної хвороби серця та цукрового діабету: вплив на біомаркери і клінічні результати
Авторы: S.V. Fedorov, O.M. Didushko, N.B. Nyshchuk-Oliinyk, N.Z. Pozur, M.V. Bielinskyi, A.S. Herashchenko
Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
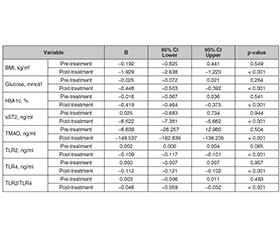
Актуальність. Серцево-судинні захворювання, такі як ішемічна хвороба серця (ІХС), є основною глобальною проблемою охорони здоров’я, що призводить до мільйонів смертей щороку. Цукровий діабет 2-го типу (ЦД2) погіршує наслідки для людей з ІХС. Спільні фактори ризику потребують синергічних підходів до лікування, включаючи використання природного флавоноїду кверцетину. Мета: вивчити клінічну ефективність та безпеку емпагліфлозину й кверцетину в лікуванні коморбідного перебігу ішемічної хвороби серця і цукрового діабету 2-го типу з урахуванням їхнього впливу на показники запалення. Матеріали та методи. У період з січня по грудень 2023 року під спостереженням перебувало 128 пацієнтів із діагнозом стабільної ІХС та ЦД2. Учасники були розподілені на три групи: першу (контроль, n = 40) — стандартне лікування ІХС та ЦД2, другу (n = 46) — стандартна терапія та емпагліфлозин (10 мг/добу), третю (n = 42) — стандартна терапія та емпагліфлозин (10 мг/добу) і кверцетин (80 мг тричі на добу). Результати. Вік і стать були подібними між групами, що свідчить про збалансований розподіл. Далі в дослідженні оцінювали вплив лікування на різні параметри. Вихідні показники індексу маси тіла (ІМТ), рівні глюкози, глікованого гемоглобіну (HbA1c), sST2, Toll-подібного рецептора-2 (TLR2) та TLR4 були порівнянними в усіх групах. Після лікування спостерігалося значне зниження ІМТ, рівнів глюкози натще, HbA1c, sST2 та співвідношення TLR2/TLR4 в усіх групах. Найбільш значущими покращення були в третій групі (емпагліфлозин і кверцетин). Отримані дані підкреслюють потенційні переваги цих втручань у пацієнтів з ішемічною хворобою серця та цукровим діабетом 2-го типу. Висновки. Додавання емпагліфлозину та кверцетину до стандартної терапії має значні переваги в управлінні ІМТ, маркерами запалення та глікемічному контролі в пацієнтів з ІХС та ЦД2. Комбінована схема лікування має потенціал щодо регулювання складної взаємодії метаболічних та запальних процесів у пацієнтів із високим ризиком. Запропонована комбінація також показала ефективність у зменшенні міокардіального стресу, що проявляється зниженням рівня сироваткового sST2.
Background. Cardiovascular diseases like coronary artery disease (CAD) are a major global health issue, causing millions of deaths each year. Type 2 diabetes mellitus (T2DM) worsens outcomes for those with CAD. Common risk factors suggest potential synergistic treatment approaches, including the use of quercetin, a natural flavonoid. The purpose was to examine the clinical efficacy and safety of empagliflozin and quercetin in the treatment of coronary artery disease and type 2 diabetes mellitus comorbidity in the light of their impact on parameters of inflammation. Materials and methods. A total of 128 patients diagnosed with both stable CAD and T2DM were enrolled in the study between January and December 2023. Participants were categorized into three groups. Group 1 (controls): 40 patients receiving the standard treatment protocol for CAD and T2DM. Group 2: 46 patients received standard therapy in addition to empagliflozin (10 mg daily). Group 3: 42 patients received standard therapy in addition to empagliflozin (10 mg daily) and quercetin (80 mg three times a day). Results. The results showed that age and gender were similar between the groups, indicating a balanced distribution. The study then evaluated the effects of treatment on various parameters. The baseline body mass index (BMI), glucose, glycated hemoglobin (HbA1c), soluble suppression of tumorigenicity 2 (sST2), Toll-like receptor 2 (TLR2) and TLR4 levels were comparable across all groups. After treatment, significant reductions were observed in BMI, fasting glucose, HbA1c, sST2, and TLR2/TLR4 in all groups. The most significant improvements were seen in the group that received both empagliflozin and quercetin. The findings highlight the potential benefits of these interventions in patients with coronary heart disease and type 2 diabetes mellitus. Conclusions. The addition of empagliflozin and quercetin to standard therapy appears to offer significant benefits in managing BMI, glycemic control, and inflammatory markers in patients with CAD and T2DM. The combined treatment regimen has potential to address the complex interplay of metabolic and inflammatory processes in high-risk patients. The proposed combination also showed efficacy in reducing the myocardial stress, which is shown by a decrease in serum sST2.
iшемічна хвороба серця; цукровий діабет; запалення; кверцетин; емпагліфлозин
coronary artery disease; diabetes mellitus; inflammation; quercetin; empagliflozin
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Lindstrom M, DeCleene N, Dorsey H, Fuster V, Johnson CO, et al. Global Burden of Cardiovascular Diseases and Risks Collaboration, 1990–2021. J Am Coll Cardiol. 2022;80(25):2372-425. doi: 10.1016/j.jacc.2022.11.001.
- Van Melle JP, Bot M, de Jonge P, de Boer RA, van Veldhui–sen DJ, Whooley MA. Diabetes, Glycemic Control, and New-Onset Heart Failure in Patients With Stable Coronary Artery Disease. Diabetes Care. 2010;33(9):2084-9. doi: 10.2337/dc10-0286.
- Serhiyenko V, Serhiyenko O. Diabetes mellitus and arte–rial hypertension. International Journal of Endocrinology (Ukraine). 2021;17(2):175-188. doi: 10.22141/2224-0721.17.2.2021.230573.
- Pankiv V. Glucocentric and cardiocentric approaches to achieving type 2 diabetes compensation. International Journal of Endocrinology (Ukraine). 2023;19(5):344-348. doi: 10.22141/2224-0721.19.5.2023.1297.
- Mykhailovska NS, Kulynych TO, Shershnova OV, Bazun YeI, Bocharnykova IS, et al. Peculiarities of clinical and metabolic profile of patients with coronary artery disease associated with type 2 diabetes mellitus (retrospective analysis). Pathologia. 2020;2. doi: 10.14739/2310-1237.2020.2.212754.
- Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021 Nov 30;144(22):e368-e454. doi: 10.1161/CIR.0000000000001029.
- Ji M, Ren D, Dunbar-Jacob J, Gary-Webb TL, Erlen JA. Self-Management Behaviors, Glycemic Control, and Metabolic Syndrome in Type 2 Diabetes. Nurs Res. 2020 Mar/Apr;69(2):E9-E17. doi: 10.1097/NNR.0000000000000401.
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, et al.; ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020 Jan 14;41(3):407-477. doi: 10.1093/eurheartj/ehz425.
- Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, et al.; ESC Scientific Document Group. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020 Jan 7;41(2):255-323. doi: 10.1093/eurheartj/ehz486.
- Jasleen B, Vishal GK, Sameera M, Fahad M, Brendan O, et al. Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors: Benefits Versus Risk. Cureus. 2023 Jan 18;15(1):e33939. doi: 10.7759/cureus.33939.
- Deepika, Maurya PK. Health Benefits of Quercetin in Age-Related Diseases. Molecules. 2022 Apr 13;27(8):2498. doi: 10.3390/molecules27082498.
- Dudek M, Kałużna-Oleksy M, Migaj J, Sawczak F, Krysztofiak H, et al. sST2 and Heart Failure-Clinical Utility and Prognosis. J Clin Med. 2023 Apr 26;12(9):3136. doi: 10.3390/jcm12093136.
- Kong P, Cui ZY, Huang XF, Zhang DD, Guo RJ, Han M. Inflammation and atherosclerosis: signaling pathways and therapeutic intervention. Signal Transduct Target Ther. 2022 Apr 22;7(1):131. doi: 10.1038/s41392-022-00955-7.
- Husain K, Hernandez W, Ansari RA, Ferder L. Inflammation, oxidative stress and renin angiotensin system in atherosclerosis. World J Biol Chem. 2015 Aug 26;6(3):209-17. doi: 10.4331/wjbc.v6.i3.209.
- Li C, Zhang J, Xue M, Li X, Han F, et al. SGLT2 inhibition with empagliflozin attenuates myocardial oxidative stress and fibrosis in diabetic mice heart. Cardiovasc Diabetol. 2019 Feb 2;18(1):15. doi: 10.1186/s12933-019-0816-2.
- Li Y, Yao J, Han C, Yang J, Chaudhry MT, et al. Quercetin, Inflammation and Immunity. Nutrients. 2016 Mar 15;8(3):167. doi: 10.3390/nu8030167.
- Chmyr N. Dynamics of endocrine and metabolic changes among patients with coronary artery disease, type 2 diabetes mellitus and metabolic syndrome while treating with telmisartan. International Journal of Endocrinology (Ukraine). 2022;18(1):22-35. doi: 10.22141/2224-0721.18.1.2022.1142.
- Kumar V, Yadav B, Nachankar A. Prevalence of Coronary Artery Disease in Asymptomatic type 2 Diabetes Mellitus Patients with Invasive Correlation in North India. Indian J Endocrinol Metab. 2023 Mar-Apr;27(2):133-139. doi: 10.4103/ijem.ijem_378_22.
- Ma CX, Ma XN, Guan CH, Li YD, Mauricio D, Fu SB. Cardiovascular disease in type 2 diabetes mellitus: progress toward perso–nalized management. Cardiovasc Diabetol. 2022 May 14;21(1):74. doi: 10.1186/s12933-022-01516-6.
- Popoviciu MS, Paduraru L, Nutas RM, Ujoc AM, Yahya G, et al. Diabetes Mellitus Secondary to Endocrine Diseases: An Update of Diagnostic and Treatment Particularities. Int J Mol Sci. 2023 Aug 11;24(16):12676. doi: 10.3390/ijms241612676.