
Журнал "Гастроэнтерология" Том 58, №2, 2024
Вернуться к номеру
Клініко-діагностичне значення трансректального ультразвукового дослідження в оцінці тяжкості виразкового коліту
Авторы: Стойкевич М.В., Титова М.В., Тарасова Т.С., Петішко О.П.
ДУ «Інститут гастроентерології НАМН України», м. Дніпро, Україна
Рубрики: Гастроэнтерология
Разделы: Клинические исследования
Версия для печати
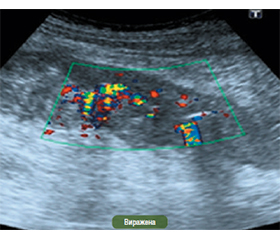
Актуальність. Вирішальну роль у діагностиці запальних захворювань кишечника (ЗЗК) відіграють ендоскопічні й гістологічні дослідження, які дозволяють підтвердити діагноз, визначити ступінь активності запального процесу, протяжність ураження кишечника і виконувати контроль перебігу ЗЗК та ефективності терапії. Проте колоноскопія не дозволяє оцінити стан усіх шарів кишечника. Краще за все з цим справляються такі сучасні неінвазивні дослідження, як ультразвукова діагностика (УЗД), комп’ютерна й магнітно-резонансна томографія. За їх допомогою можна оцінити стан стінки кишки й отримати зображення кишки в поперечному перерізі, оцінити позакишкові структури (лімфовузли, судини, жирову клітковину). Можна сказати, що ендоскопія та УЗД шукають той самий тип інформації, але дивляться на різні речі. Поглиблення знань щодо ролі УЗД дистальних відділів ободової кишки при виразковому коліті (ВК) буде сприяти поліпшенню діагностики, розробці методів визначення активності ВК, контролю терапії, що дозволить оптимізувати вибір адекватних лікувальних заходів. Мета: удосконалити діагностику виразкового коліту на підставі вивчення ультрасонографічних параметрів прямої кишки. Матеріали та методи. Трансректальне УЗД (ТРУЗД) проводилось на ультразвуковому сканері експертного класу SonoScape S60 з використанням низькочастотного конвексного датчика 3,5 МГц і ректовагінального конвексного датчика 6 МГц. Для огляду використовувались трансперинеальний і трансректальний доступи. Результати. Товщина стінки і товщина підслизового шару вірогідно відрізнялися у хворих із середнім і тяжким ступенем ВК. Аналізуючи показники ТРУЗД залежно від ендоскопічної активності ВК, вірогідних відмінностей за товщиною стінки ми не виявили. Але визначена тенденція до збільшення товщини слизового шару і коефіцієнта деформації (КД) з підвищенням ендоскопічної активності. У більшості пацієнтів визначалось підвищення ступеня щільності кровотоку, яке залежало від тяжкості захворювання. При проведенні регресійного аналізу встановлено зв’язок товщини кишкової стінки (r = 0,44; р = 0,0121) і товщини підслизового шару (r = 0,86; р = 0,006) з індексом Мейо. Встановлено кореляційний зв’язок товщини стінки товстої кишки з частотою випорожнень (r = 0,37; р = 0,018), лейкоцитозом (r = 0,38; р = 0,016) і швидкістю осідання еритроцитів (r = 0,35; р = 0,027). Щільність кровотоку кишкової стінки позитивно корелювала з наявністю набряку (r = 0,32; р = 0,045), вираженістю судинного рисунка (r = 0,42; р = 0,008), наявністю ерозій (r = 0,4; р = 0,011) і кровоточивістю слизової оболонки (r = 0,50; р = 0,001). Коефіцієнт деформації позитивно корелював з наявністю метеоризму (r = 0,35; р = 0,048). Висновки. Ендоскопічне дослідження в пацієнтів із ВК слід доповнювати ТРУЗД. Встановлено кореляційний зв’язок товщини кишкової стінки і товщини підслизового шару в пацієнтів із ВК з індексом Мейо. Визначена тенденція до збільшення товщини слизового шару і КД з підвищенням ендоскопічної активності. Встановлені взаємозв’язки між ендоскопічними й ультразвуковими показниками можуть бути використані для визначення активності захворювання.
Background. Endoscopic and histological studies play a decisive role in the diagnosis of inflammatory bowel diseases, as they allow confirming the diagnosis, determining the degree of inflammatory activity, the extent of intestinal damage, and monitoring the course of disease and the effectiveness of therapy. However, it is not possible to assess the state of all intestinal layers with colonoscopy. Modern non-invasive methods such as ultrasound, computed tomography, and magnetic resonance imaging cope best with this purpose. With their help, you can assess the state of the intestinal wall and obtain a cross-sectional image of the intestine, evaluate extraintestinal structures (lymph nodes, vessels, fatty tissue). It can be said that endoscopy and ultrasound search for the same type of information but look at different things. Deepening the knowledge about the role of ultrasound of the distal parts of the colon in ulcerative colitis (UC) will contribute to the improvement of diagnosis, development of methods for determining the activity of UC, control of therapy, which will allow optimizing the choice of adequate treatment measures. The goal of the work: to improve the diagnosis of ulcerative colitis based on the study of ultrasonographic parameters of the rectum. Materials and methods. Transrectal ultrasound was performed on an expert-class SonoScape S60 ultrasound scanner using a low-frequency convex probe of 3.5 MHz and a rectovaginal convex probe of 6 MHz. Transperineal and transrectal approaches were used. Results. Wall thickness and submucosal thickness differed significantly in moderate and severe UC. Analysis of transrectal ultrasound indicators depending on the endoscopic activity of the UC revealed no significant differences in the rectal wall thickness. But there was a tendency to increase in the thickness of the mucous layer and the coefficient of deformation with increasing endoscopic activity. Most patients had an increase in the degree of blood flow density, which depended on the disease severity. During the regression analysis, a relationship was found between the intestinal wall thickness (r = 0.44; p = 0.0121) and submucosal layer thickness (r = 0.86; p = 0.006) with the Mayo index. A correlation was revealed between the thickness of the colon wall and the frequency of bowel movements (r = 0.37; p = 0.018), leukocytosis (r = 0.38; p = 0.016) and erythrocyte sedimentation rate (r = 0.35; p = 0.027). The blood flow density in the intestinal wall positively correlated with the presence of edema (r = 0.32; р = 0.045), the severity of the vascular pattern (r = 0.42; р = 0.008), the presence of erosions (r = 0.4; р = 0.011) and bleeding of the mucous membrane (r = 0.50; p = 0.001). The coefficient of deformation positively correlated with the presence of flatulence (r = 0.35; р = 0.048). Conclusions. Endoscopic examination in patients with UC should be supplemented with transrectal ultrasound. A correlation was found between the intestinal wall thickness and the thickness of the submucosal layer in patients with UC and the Mayo index. A tendency to increase in the thickness of the mucous layer and the coefficient of deformation with increasing endoscopic activity was determined. Relationships between endoscopic and ultrasound parameters can be used to assess disease activity.
трансректальне ультразвукове дослідження; виразковий коліт; ступінь тяжкості; еластометрія кишкової стінки; доплерсканування стінки прямої кишки
transrectal ultrasound; ulcerative colitis; degree of severity; intestinal wall elastography; Doppler of the rectal wall
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Ng SC, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of po–pulation-based studies. Lancet. 2017;390(10114):2769-2778. doi: 10.1016/S0140-6736(17)32448.
- Ye Y, et al. The epidemiology and risk factors of inflammatory bowel disease. International Journal of Clinical and Experimental Medicine. 2015;8:22529-22542.
- Windsor JW, Kaplan GG. Evolving Epidemiology of IBD. Current Gastroenterology Reports. 2019;21(8):40. https://doi.org/10.1007/s11894-019-0705-6.
- Guan QA. Comprehensive Review and Update on Pathogenesis of Inflammatory Bowel Disease. Journal of Immunology Research. 2019; 2019:7247238. doi: 10.1155/2019/7247238.
- Li S, Zhang F, Zhang Q. Pathological features-based targeted delivery strategies in IBD therapy: A mini review. Biomedicine & Pharmacotherapy = Biomedecine & Pharmacotherapie. 2022;151:113079. https://doi.org/10.1016/j.biopha.2022.113079.
- Dolinger MT, et al. Current and Novel Uses of Intestinal Ultrasound in Inflammatory Bowel Disease. Gastroenterol Hepatol (NY). 2023;19(8):447-457. PMID: 37772159; PMCID: PMC10524432.
- Fábián A, Bor R, Szepes Z. The use of ultrasound in colonic and perianal diseases. Curr Opin Gastroenterol. 2023;39(1):50-56. doi: 10.1097/MOG.0000000000000891.
- Bavil AS, et al. Ultrasonographic evaluation of bowel wall thickness and intramural blood flow in ulcerative colitis. Gastroenterol. 2012;370495. doi:10.5402/2012/370495.
- Allocca M, et al. Point of Care Ultrasound in Inflammatory Bowel Disease. J Crohns Colitis. 2021;15(1):143-151. doi: 10.1093/ecco-jcc/jjaa151. PMID: 32674146.
- Wang L, et al. Utilization of Ultrasonic Image Characteristics Combined with Endoscopic Detection on the Basis of Artificial Intelligence Algorithm in Diagnosis of Early Upper Gastrointestinal Cancer. J Healthc Eng. 2021;2773022:1-5. doi: 10.1155/2021/2773022.
- Wang G, et al. EFSUMB Recommendations and Clinical Guidelines for Intestinal Ultrasound (GIUS) in Inflammatory Bo–wel Diseases. EFSUMB-Empfehlungen und klinische Leitlinien für den gastrointestinalen Ultraschall (GIUS) chronisch entzündlichen Darmerkrankungen (CED). Ultraschall Med. 2018;39(3):304-317. doi: 10.1055/s-0043-125329.
- Allocca M, et al. Accuracy of Humanitas Ultrasound Criteria in Assessing Disease Activity and Severity in Ulcerative Colitis: A Prospective Study. J Crohns Colitis. 2018;12(12):1385-1391. doi: 10.1093/ecco-jcc/jjy107.
- Bryant RV, et al Gastrointestinal ultrasound in inflammatory bowel disease: an underused resource with potential paradigm-chan–ging application. Gut. 2018;67(5):973-85.
- Iglesias-García J, Domínguez-Muñoz JE. A new open door for endoscopic ultrasound (EUS); the colon. The Spanish Journal of Gastroenterology. 2015;8:467-468. DOI: 10.17235/reed.2015.3927/2015.
- Allocca M, et al. Point-of-Care Ultrasound in Inflammatory Bowel Disease. Journal of Crohn’s and Colitis. 2021 Jan 13;15(1):143-151. doi: 10.1093/ecco-jcc/jjaa151.
- Martínez Pérez MJ, Blanc García E, Merino Bonilla JA. Bowel ultrasound: examination techniques and normal and pathologic patterns. Ecografía intestinal: técnicas de examen, patrones normales y patológicos. Radiologia (Engl Ed). 2020;62(6):517-527. doi:10.1016/j.rx.2020.09.004.
- Allocca M, et al. Milan ultrasound criteria are accurate in assessing disease activity in ulcerative colitis: external validation. United European Gastroenterol J. 2021;9(4):438-442. doi: 10.1177/2050640620980203.
- Allocca M, et al. Predictive value of Milan ultrasound criteria in ulcerative colitis: A prospective observational cohort study. United European Gastroenterol J. 2022;10(2):190-197. doi: 10.1002/ueg2.12206.
- Ripollés T, et al. Evaluation of Crohn’s Disease Activity: Development of an Ultrasound Score in a Multicenter Study. Inflamm Bowel Dis. 2021;27(1):145-154. doi: 10.1093/ibd/izaa134.
- Stenczel ND. The role of the intestinal ultrasound in Crohn’s disease diagnosis and monitoring. J Med Life. 2021;14(3):310-315. doi: 10.25122/jml-2021-0067.
- Savik F, et al. Development and Validation of a Simple Ultrasound Activity Score for Crohn’s Disease. J Crohns Colitis. 2021;15(1):115-124. doi: 10.1093/ecco-jcc/jjaa112.
- Roushan N, et al. Differentiation of Crohn’s disease and ulcerative colitis using intestinal wall thickness of the colon: A Diagnostic accuracy study of endoscopic ultrasonography. Med J Islam Repub Iran. 2019;33:57. doi: 10.34171/mjiri.33.57.
- Amr M, et al. Value of endoscopic ultrasound in prediction of dysplasia in ulcerative colitis. The Egyptian Journal of Internal Medi–cine. 2019;31:480-486.
- Ishikawa D, et al. Images of colonic real-time tissue sonoelastography correlate with those of colonoscopy and may predict response to therapy in patients with ulcerative colitis. BMC Gastroenterol. 2011;11:29. https://doi.org/10.1186/1471-230X-11-29.
- Andrzejewska M, Grzymislawski M. The role of intestinal ultrasound in diagnostics of bowel diseases. Prz Gastroenterol. 2018;(1):1-5. doi: 10.5114/pg.2018.74554.
- Statie RC, et al. The Use of Endoscopic Ultrasonography in Inflammatory Bowel Disease: A Review of the Literature. Diagnostics (Basel). 2023 Feb 3;13(3):568. doi: 10.3390/diagnostics13030568. PMID: 36766671; PMCID: PMC9914551.
- Gast P, Belaïche J. Rectal endosonography in inflammatory bowel disease: Differential diagnosis and prediction of remission. Endoscopy. 1999;31:158-166. doi: 10.1055/s-1999-13665.
- Rasmussen SN, Riis P. Rectal wall thickness measured by ultrasound in chronic inflammatory diseases of the colon. Scand. J. Gastroenterol. 1985;20:109-114. doi: 10.3109/00365528509089641.
- Dağli U, Over H, Tezel A, Ulker A, Temuçin G. Transrectal ultrasound in the diagnosis and management of inflammatory bowel disease. Endoscopy. 1999;31:152-157. doi: 10.1055/s-1999-13664.
- Rana SS, Kante B, Shah J, Nada R, Kalra N, Gupta R. Role of EUS in idiopathic ulcerative colitis. Endosc Ultrasound. 2021;10:313-314. doi: 10.4103/EUS-D-20-00224.
- Cho E, Mochizuki N, Ashihara T, Yasuda K, Nakajima M. Endoscopic ultrasonography in the evaluation of inflammatory bo–wel disease. Endoscopy. 1998;30(1):A94-A96. doi: 10.1055/s-2007-1001484.
- Cho E, Yasuda K, Nakajima M. EUS in the diagnosis of ulcerative colitis. Dig Endosc. 2004;16:S182-S184. doi: 10.1111/j.1443-1661.2004.00445.x.
- Yan B, et al. Reliability of EUS indices to detect inflammation in ulcerative colitis. Gastrointest. Endosc. 2017;86:1079-1087. doi: 10.1016/j.gie.2017.07.035.
- Jin RF, Chen YM, Chen RP, Ye HJ. Endoscopic ultrasonography in the evaluation of condition and prognosis of ulcerative colitis. World J Clin. Cases. 2022;10:4818-4826. doi: 10.12998/wjcc.v10.i15.4818.
- Watanabe O, et al. Role of endoscopic ultrasonography in predicting the response to cyclosporin A in ulcerative colitis refractory to steroids. Dig Liver Dis. 2009;41:735-739. doi: 10.1016/j.dld.2009.03.014.
- Yoshizawa S, Kobayashi K, Katsumata T, Saigenji K, Okayasu I. Clinical usefulness of EUS for active ulcerative colitis. Gastrointest. Endosc. 2007;65:253-260. doi: 10.1016/j.gie.2005.10.037.
- Castellano MA, Scheeffer V, Petersen V, da Silveira TR. Evaluation of bowel wall flow by color Doppler ultrasound in the assessment of inflammatory bowel disease activity in pediatric patients. Radiol Bras. 2023 Sep-Oct;56(5):242-247. doi: 10.1590/0100-3984.2023.0039-en.
- Rustemovic N, et al. A pilot study of transrectal endoscopic ultrasound elastography in inflammatory bowel disease. BMC Gastroenterol. 2011;11:113. doi: 10.1186/1471-230X-11-113.