Резюме
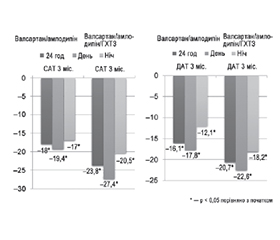
Актуальність. Використання фіксованих комбінацій антигіпертензивних препаратів може поліпшити контроль АТ та зменшити ускладнення і збільшити тривалість життя. Метою нашого дослідження було проаналізувати ефективність фіксованих, вільних та нетрадиційних комбінацій антигіпертензивних препаратів у лікуванні пацієнтів із АГ. Матеріали та методи. Обстежено 396 пацієнтів із артеріальною гіпертензією різного ступеня тяжкості. Критеріями включення були вік пацієнтів старше за 18 років та рівень офісного АТ більше ніж 140/90 мм рт.ст. Пацієнти були в трьох групах спостереження: традиційні вільні комбінації, традиційні фіксовані комбінації та нетрадиційні вільні комбінації. 91 пацієнт з АГ, що отримував нефіксовану комбінацію раміприлу та гідрохлортіазиду (ГХТЗ), був розподілений для вивчення її впливу на зниження АТ, переносимість та побічні ефекти; 132 пацієнти з АГ, що отримували нефіксовану комбінацію метопрололу ретард та гідрохлортіазиду, — її впливу на АТ, переносимість та розвиток побічних реакцій; 50 пацієнтів — для вивчення впливу фіксованих традиційних подвійних та потрійних комбінацій антигіпертензивних препаратів на зниження АТ; 123 пацієнти — у групу вивчення впливу дигідропіридинових і недигідропіридинових антагоністів кальцію на ступінь зниження артеріального тиску та розвиток побічних реакцій. Результати. Використання метопрололу пролонгованої дії в дозі 100–300 мг на день у хворих на м’яку та помірну артеріальну гіпертензію забезпечувало достовірне зниження як офісного САТ на 32 мм рт.ст., ДАТ — на 18 мм рт.ст., ЧСС — на 18 уд/хв, так і середньодобового САТ — на 21 мм рт.ст., ДАТ — на 13 мм рт.ст. та ЧСС — на 7 уд/хв та сприяло досягненню цільового АТ у 93,6 % — за даними офісного вимірювання, а за даними ДМАТ — у 84,9 % випадків. Використання раміприлу (10 мг) у комбінації з гідрохлортіазидом (25 мг) у хворих з м’якою та помірною артеріальною гіпертензією забезпечувало достовірне зниження як офісного САТ на 36,6 мм рт.ст., ДАТ — на 17,2 мм рт.ст., так і 24САТ — на 18,9 мм рт.ст. і 24ДАТ — на 7,0 мм рт.ст. Призначене лікування найліпше переносилося хворими, що приймали монотерапію лерканідипіном 20 мг або низькодозову комбінацію лерканідипіну 10 мг та дилтіазему 120 мг. За даними офісного та добового моніторування АТ, комбіноване лікування на основі лерканідипіну і дилтіазему було таке ж ефективне, як і монотерапія лерканідипіном і дилтіаземом. На фоні фіксованої потрійної комбінації валсатан/ГХТЗ/амлодипін зниження 24САТ/ДАТ становило –23,8/20,7 мм рт.ст., а зниження АТ за денний та нічний періоди становило –27,4/22,6 та –20,5/18,2 мм рт.ст. відповідно (р < 0,05 для усіх значень). Досягнення цільового рівня АТ при добовому моніторуванні відзначено у групі фіксованої подвійної терапії валсартн/амлодипін — у 77,3 %, у групі потрійної комбінації валсартн/амлодипін/гідрохлортіазид — у 95,2 % пацієнтів. Висновки. Потрійна фіксована комбінація валсартан/ГХТЗ/амлодипін була найефективнішою в зниженні АТ, що сприяло досягненню цільових рівнів АТ при офісному вимірюванні у 95,7 %, при ДМАТ — у 95,2 % випадків.
Background. The use of fixed combinations of antihypertensive drugs can improve blood pressure (BP) control, reduce complications, and increase life expectancy. The aim of our study was to analyze the effectiveness of fixed, free, and unconventional combinations of antihypertensive drugs in the treatment of patients with hypertension. Materials and methods. We have examined 396 patients with hypertension of varying severity. The inclusion criteria were the age of patients above 18 years and the level of office BP greater than 140/90 mmHg. Patients were divided into three observation groups: traditional free combinations, traditional fixed combinations, and unconventional free combinations. Ninety-one patients with hypertension who received an unfixed combination of ramipril and hydrochlorothiazide (HCTZ) were randomized to study its effect on BP reduction, tolerability, and side effects; 132 hypertensive patients who took an unfixed combination of metoprolol retard and hydrochlorothiazide — its effect on blood pressure, tolerability and development of adverse reactions; 50 patients — to study the effect of traditional fixed double and triple combinations of antihypertensive drugs on BP reduction; 123 patients — in the group of studying the effect of dihydropyridine and non-dihydropyridine calcium antagonists on the degree of blood pressure reduction and the development of adverse reactions. Results. The use of long-acting metoprolol in a dose of 100–300 mg/day in patients with mild and moderate hypertension ensured a significant decrease in office systolic blood pressure (SBP) — by 32 mmHg, diastolic blood pressure (DBP) — by 18 mmHg, heart rate — by 18 bpm, the average daily SBP — by 21 mmHg, DBP — by 13 mmHg, heart rate — by 7 bpm and contributed to the achievement of target BP in 93.6 % of cases according to office measurement, and in 84.9 % patients according to ambulatory blood pressure monitoring. The use of ramipril (10 mg) in combination with hydrochlorothiazide (25 mg) in patients with mild and moderate hypertension provided a reliable reduction of office SBP — by 36.6 mmHg, DBP — by 17.2 mmHg, SBP24 — by 18.9 mmHg, DBP24 — by 7.0 mmHg. The prescribed treatment was most effective in patients taking monotherapy with lercanidipine 20 mg or a low-dose combination of lercanidipine 10 mg and diltiazem 120 mg. According to the office and daily BP monitoring, a combined treatment based on lercanidipine and diltiazem was as effective as monotherapy with lercanidipine and dil-tiazem. When using a triple fixed combination of valsartan/HCTZ/amlodipine, a decrease in SBP24/DBP24 was 23.8/20.7 mmHg, and a decrease in BP during the day and night periods was 27.4/22.6 and 20.5/18.2 mmHg, respectively (р < 0.05 for all values). The target BP level during daily monitoring was achieved in 77.3 % of cases in the group of a double fixed therapy of valsartan/amlodipine, and in 95.2 % in the group of a triple combination of valsartan/amlodipine/hydrochlorothiazide. Conclusions. A triple fixed combination of valsartan/HCTZ/amlodipine was the most effective in lowering BP, which contributed to the achievement of target blood pressure levels at office measurement in 95.7 %, at ambulatory blood pressure monitoring — in 95.2 % of patients.
Список литературы
1. Рековець О.Л., Сіренко Ю.М., Торбас О.О., Кушнір С.М., Примак Г.Ф. Використання фіксованих подвійних і потрійних комбінацій у досягненні цільового рівня артеріального тиску при добовому моніторуванні у пацієнтів з артеріальною гіпертензією. Буковинський медичний вісник. 2020. № 2 (94). С. 102-112. doi: 10.24061/2413-0737. XXIV.2.94.2020.50.
2. Сіренко Ю.М., Рековець О.Л., Доброход А.С. Оцінка впливу моно- та комбінованої антигіпертензивної терапії дигідропіридиновими та недигідропіридиновими антагоністами кальцію на показники офісного артеріального тиску та артеріального тиску при добовому моніторуванні у пацієнтів із м’якою та помірною артеріальною гіпертензією. Артеріальна гіпертензія. 2016. Т. 1 (45). С. 45-66.
3. Сиренко Ю.Н., Рековец О.Л. Влияние метопролола ретарда на утренний подъем артериального давления у пациентов с мягкой и умеренной артериальной гипертензией по данным суточного мониторирования артериального давления. Український кардіологічний журнал. 2006. № 3. С. 73-77.
4. Сиренко Ю.Н., Рековец О.Л., Андриевская С.А., Бабак О.Я., Говорова О.В., Рудык Ю.С. Антигипертензивная эффективность рамиприла у больных с мягкой и умеренной артериальной гипертензией (результаты многоцентрового исследования RASH — RАmipril Study in patient with arterial Hypertension). Український кардіологічний журнал. 2007. № 1. С. 41-47.
5. Allemann Y, Fraile B, Lambert M, et al. Efficacy of the combination of amlodipine and valsartan in patients with hypertension uncontrolled with previous monotherapy: the Exforge in Failure after Single Therapy (EX-FAST) study. J Clin Hypertens (Greenwich). 2008;10:185-194.
6. Baser O, Andrews LM, Wang L, Xie L. Comparison of real world adherence, healthcare resource utilization and costs for newly initiated valsartan/amlodipine single-pill combination versus angiotensin receptor blocker/calcium channel blocker free combination therapy. J Med Econ. 2011;14:576-83.
7. Boggia J, Li Y, Thijs L, et al. Prognostic accuracy of day versus night ambulatory blood pressure: a cohort study. Lancet. 2007;370:1219-1229.
8. Boutouyrie P, Achouba A, Trunet P, Laurent S; EXPLOR Trialist Group. Amlodipine-valsartan combination decreases central systolic blood pressure more e ectively than the amlodipine-atenolol combination: the EXPLOR study. Hypertension. 2010; 55:1314-1322.
9. Calhoun DA, Crikelair NA, Yen J, Glazer RD. Amlodipine/valsartan/hydrochlorothiazide triple combination therapy in moderate/severe hypertension: secondary analyses evaluating efficacy and safety. Adv Ther. 2009;26:1012-23.
10. Calhoun DA, Lacourciere Y, Crikelair N, Jia Y, Gla-zer RD. Effects of demographics on the antihypertensive efficacy of triple therapy with amlodipine, valsartan, and hydrochlorothiazide for moderate to severe hypertension. Curr Med Res Opin. 2013;29:901-10.
11. Dahlof B, Hansson L, Lindholm LH et al. Swedish trial in old patients with hypertension (STOP-Hypertension): analyses performed up to l992. Clin. Exp. Hypertens. 1993;15:925-39.
12. Dahlof B, Lindholm LH, Hansson L et al. Morbidity and mortality in the Swedish Trial in Old Patients with Hypertension (STOP-Hypertension). Lancet. 1991;338:1281-1285.
13. Destro M, Luckow A, Samson M, Kandra A, Brunel P. Efficacy and safety of amlodipine/valsartan compared with amlodipine monotherapy in patients with stage 2 hypertension: a randomized, double-blind, multicenter study: the EX-EFFeCTS Study. J Am Soc Hypertens. 2008;2:294-302.
14. DREAM Trial Investigators; Bosch J, Yusuf S, Gerstein HC, Pogue J, Sheridan P, Dagenais G, et al. Effect of ramipril on the incidence of diabetes. N. Engl. J. Med. 2006;12:1551-1562.
15. Flack JM, Calhoun DA, Satlin L, Barbier M, Hilkert R, Brunel P. Efficacy and safety of initial combination therapy with amlodipine/valsartan compared with amlodipine monotherapy in black patients with stage 2 hypertension: the EX-STAND study. J Hum Hypertens. 2009;23:479-89.
16. Genth-Zotz S, Zotz R, Sigmund M et al. MIC Trial: Metoprolol in patients with mild to moderate heart failure: effects on ventricular function and cardiopulmonary exercise testing. Europ. J. Heart Failure. 2000;2:175-181.
17. Johannesson M, Dahlof B, Lindholm LH et al. The cost-effectiveness of treating hypertension in elderly people — an analysis of the Swedish Trial in Old Patients with Hypertension (STOP-Hypertension). J. Intern. Med. 1993;234:317-323.
18. Jorge Sison, Rosa María Ríos Vega, Hu Dayi, Giovanni Bader & Patrick Brunel. Efficacy and effectiveness of valsartan/amlodipine and valsartan/amlodipine/hydrochlorothiazide
in hypertension: randomized-controlled versus observational studies. Current Medical Research and Opinion. DOI: 10.1080/03007995.2017.1412682.
19. Kafrawy NE, Rashwan M, Lion K, Khedr K, Nashaat N. Effectiveness and tolerability of fixed dose combination of amlodipine/valsartan in treatment of hypertension in the real-life setting among Egyptian patients. Egyptian Heart J. 2014;66:30-5.
20. Kario K, Tomitani N, Kanegae H, Ishii H, Uchiyama K, Yamagiwa K, et al. Comparative e ects of an angiotensin II receptor blocker (ARB)/diuretic vs. ARB/calcium-channel blocker combination on uncontrolled nocturnal hypertension evaluated by information and communication technology-based nocturnal home blood pressure monitoring — the NOCTURNE Study. Circ J. 2017;81:948-957.
21. Khan W, Moin N, Iktidar S, Sakrani J, Abid R, Afzal J, et al. Real-life effectiveness, safety, and tolerability of amlodipine/valsartan or amlodipine/valsartan/hydrochlorothiazide singlepill combination in patients with hypertension from Pakistan. Ther Adv Cardiovasc Dis. 2014;8:45-55.
22. Kjekshus JK. According to MIAMI and ISIS-1 trials, can a general recommendation be given for beta blockers in acute myocardial infarction? Cardiovasc. Drugs Ther. 1988;2:113-119.
23. LaPalio L, Schork A, Glasser S et al. Safety and efficacy of metoprolol in treatment of hypertension in the elderly. J. Am. Geriatr. Soc. 1992;40:354-358.
24. Lash JP, Wang X, Greene T, Gadegbeku CA, Hall Y, Jones K, et al.; African American Study of Kidney Disease and Hypertension Trial Study Group. Quality of life in the African American Study of Kidney Disease and Hypertension: effects of blood pressure management. Am. J. Kidney Dis. 2006;47:956-964.
25. Lins R, Aerts A, Coen N, Hermans C, MacDonald K, Brie H, et al. Effectiveness of amlodipine-valsartan single-pill combinations: hierarchical modeling of blood pressure and total cardiovascular disease risk outcomes (the EXCELLENT study). Ann Pharmacother. 2011;45:727-39.
26. Luomanmaki K, Inkovaara J, Hartikainen M et al. Efficacy and tolerability of isradipine and metoprolol in treatment of hypertension: the Finnish Isradipine Study in Hypertension (FISH). J. Cardiovasc. Pharmacol. 1992;20:296-303.
27. Mallat SG, Itani HS, Tanios BY. Current perspectives on combination therapy in the management of hypertension. Integr Blood Press Control. 2013;6:69-78.
28. Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Bohm M, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31:1281-357.
29. Marre M, Lievre M, Chatellier G, Mann JF, Passa P, Menard J; DIABHYCAR Study Investigators. Effect of low dose ramipril on cardiovascular and renal outcomes in patients with type 2 diabetes and raised excretion of urinary albumin: randomised, double blind, placebo controlled trial (the DIABHYCAR study). BMJ. 2004;28:495.
30. Matsui Y, Eguchi K, O’Rourke MF, Ishikawa J, Miyashita H, Shimada K, Kario K. Differential effects between a calcium channel blocker and a diuretic when used in combination with angiotensin II receptor blocker on central aortic pressure in hypertensive patients. Hypertension. 2009;54:716-723.
31. Oparil S, Giles T, Ofili EO., Pitt B, Seifu Y, Hil-kert R, Samuel R, Sowers JR. Moderate versus intensive treatment of hypertension with amlodipine/valsartan for patients uncontrolled on angiotensin receptor blocker monotherapy. J Hypertens. 2011 Jan;29(1):161-170. doi: 10.1097/HJH.0b013e32834000a7.
32. Philipp T, Smith TR, Glazer R, Wernsing M, Yen J, Jin J, et al. Two multicenter, 8-week, randomized, double-blind, placebocontrolled, parallel-group studies evaluating the efficacy and tolerability of amlodipine and valsartan in combination and as monotherapy in adult patients with mild to moderate essential hypertension. Clin Ther. 2007;29:563-80.
33. Pogue V, Rahman M, Lipkowitz M, et al. Disparate estimates of hypertension control from ambulatory and clinic blood pressure measurements in hypertensive kidney disease. Hypertension. 2009;53:20-27.
34. Samir H Assaad-Khalil, Nashwa Nashaat. Real-life Effectiveness and Safety of Amlodipine/Valsartan Single-pill Combination in Patients with Hypertension in Egypt: Results from the EXCITE Study. Drugs — Real World Outcomes. 2016;3:307-315. DOI: 10.1007/s40801-016-0082-5.
35. Sawada T, Yamada H, Dahlf B and Matsubara H, for the KYOTO HEART Study Group. Effects of valsartan on morbidity and mortality in uncontrolled hypertensive patients with high cardiovascular risks: KYOTO HEART Study. Eur. Heart J. 2009;30:2461-2469.
36. Schrader J, Luders S, Kulschewski A, Hammersen F, Zuchner C, Venneklaas U, et al.; MARPLE Study Group. Microalbuminuria and tubular proteinuria as risk predictors of cardiovascular morbidity and mortality in essential hypertension: final results of a prospective long-term study (MARPLE Study). J. Hypertens. 2006;24:541-548.
37. Sison J, Assaad-Khalil SH, Najem R, Kitchlew AR, Cho B, Ueng KC, et al. Real-world clinical experience of amlodipine/valsartan and amlodipine/valsartan/hydrochlorothiazide in hypertension: the EXCITE study. Curr Med Res Opin. 2014;30:1937-45.
38. Waeber B, Ruilope LM Amlodipine and valsartan as components of a rational and effective fixed-dose combination. Vasc Health Risk Manag. 2009;5:165-174.
39. Weycker D, Keskinaslan A, Levy DG, et al. Effectiveness of add-on therapy with amlodipine in hypertensive patients recei-ving valsartan. Blood Press Suppl. 2008;2:5-12.
40. White W. Blood pressure monitoring in cardiovascular medicine and therapeutics. New Jersey: Humana Press, 2001. 308 p.