
Журнал «Травма» Том 26, №1, 2025
Вернуться к номеру
Скінченно-елементне моделювання й оптимізація біомеханічних параметрів короткої стабілізації вибухових переломів грудопоперекового переходу при компресійному навантаженні
Авторы: Нехлопочин О.С. (1), Вербов В.В. (1), Чешук Є.В. (1), Карпінський М.Ю. (2), Яресько О.В. (2), Корольков І.О. (3)
(1) - ДУ «Інститут нейрохірургії імені академіка А.П. Ромоданова НАМН України», м. Київ, Україна
(2) - ДУ «Інститут патології хребта та суглобів імені професора М.І. Ситенка НАМН України», м. Харків, Україна
(3) - Харківський національний університет радіоелектроніки, м. Харків, Україна
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
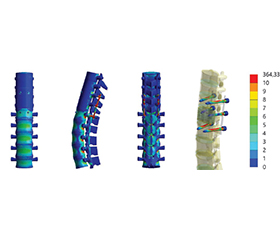
Актуальність. Вибухові переломи (ВП) становлять до 15–20 % травм грудопоперекового відділу, причому 40–50 % із них локалізуються саме на рівні грудопоперекового переходу (ГПП). Виникає потреба у розробці оптимальної стратегії лікування потерпілих із ВП ділянки ГПП. Одним із компромісних рішень є методика встановлення «проміжних» гвинтів безпосередньо у вражений хребець. Питання біомеханічної доцільності використання таких гвинтів у структурі короткої фіксації, а також підбору довжини основних гвинтів системи досі залишається відкритим. Мета: вивчити напружено-деформований стан моделі грудопоперекового відділу хребта із ВП хребця Тh12 при коротких варіантах транс-педикулярної фіксації та доцільність використання проміжних гвинтів. Матеріали та методи. Розроблена математична скінченно-елементна модель грудопоперекового відділу хребта людини з ВП хребця Тh12. Змодельовано чотири варіанти транспедикулярної фіксації двох суміжних із ушкодженим хребців. У двох моделях використовували короткі та довгі фіксувальні гвинти без додаткових коротких проміжних гвинтів у тіло Th12. У двох інших моделях додатково встановлювали по два короткі гвинти у хребець Th12. Напружено-деформований стан моделей досліджували під впливом вертикального стискаючого розподіленого навантаження величиною 350 Н. Результати. З короткою фіксацією установка проміжних гвинтів у переломний хребець Th12 додатково стабілізує його тіло, що особливо відчутно у моделях із монокортикальними гвинтами на рівнях Th11 і L1. Якщо без проміжних гвинтів у тілі Th12 напруження могли сягати 9,7 МПа, то з додатковими гвинтами вони зазвичай зменшуються до 8,5–9,0 МПа. Перехід до бікортикальних гвинтів у поєднанні із проміжними гвинтами здатен ще більше знижувати навантаження у пошкодженому хребці — до 8,1 МПа, але зумовлює зростання навантажень на самі гвинти та місця їх входу. При цьому в опорних балках зазвичай фіксується приблизно 220–230 МПа замість 240–250, що все ж нижче, ніж у варіанті без проміжних гвинтів, але недостатньо для рівномірного розподілу навантажень. Висновки. Порівняльний аналіз варіантів короткої фіксації ВП зони ГПП при осьовому компресійному навантаженні з урахуванням наявності проміжних гвинтів і вибору моно- чи бікортикальних гвинтів свідчить, що найбільш сприятливих результатів вдається досягти у разі встановлення проміжних гвинтів у тіло ушкодженого хребця та використання бікортикальних гвинтів на суміжних рівнях. Така конфігурація дає змогу знизити пікові напруження у зоні перелому й у місцях входу гвинтів, що зменшує ймовірність прогресування деформації та розхитування імплантів.
Background. Burst fractures account for up to 15–20 % of thoracolumbar injuries, with 40–50 % of them localized at the level of the thoracolumbar junction. There is a need to develop optimal treatment strategy for victims with burst fractures of the thoracolumbar junction. One of the compromise solutions is the insertion of intermediate screws directly in the affected vertebra. The question of the biomechanical feasibility of using such screws in the structure of short fixation, as well as the selection of the length of the main screws of the system remains open. Objective: to study the stress-strain state of the model of the thoracolumbar spine with a burst fracture of the Th12 vertebra with short variants of transpedicular fixation and the feasibility of using intermediate screws. Materials and methods. A mathematical finite element model of the human thoracolumbar spine with a burst fracture of the Th12 vertebra was developed. Four variants of transpedicular fixation of two adjacent vertebrae to the damaged one were simulated. In two models, short and long fixing screws were used without additional short intermediate screws into the Th12 body. In the other two models, two short screws were additionally installed into the Th12 vertebra. The stress-strain state of the models was investigated under a vertical compressive distributed load of 350 N. Results. With short fixation, the installation of intermediate screws into the fractured Th12 vertebra additionally stabilizes its body, which is especially noticeable in models with monocortical screws at the Th11 and L1 levels. If without intermediate screws the stresses in the Th12 body could reach 9.7 MPa, then with additional screws, they usually decrease to 8.5–9.0 MPa. The transition to bicortical screws in combination with intermediate screws can further reduce the load in the damaged vertebra — up to 8.1 MPa, but causes an increase in the loads on the screws themselves and their entry points. At the same time, approximately 220–230 MPa instead of 240–250 is usually fixed in the support beams, which is still lower than in the variant without intermediate screws, but not enough for uniform load distribution. Conclusions. A comparative analysis of options for short fixation of burst fractures of the thoracolumbar junction under axial compression load, taking into account the presence of intermediate screws and the choice of mono- or bicortical screws, shows that the most favorable outcomes can be achieved when intermediate screws are installed in the body of the damaged vertebra and bicortical screws are used in adjacent levels. This configuration allows you to reduce peak stresses in the fracture zone and at the screw entry points, which reduces the likelihood of deformity progression and loosening of implants.
хребет; грудопоперековий перехід; транспедикулярна фіксація
spine; thoracolumbar junction; transpedicular fixation