
Международный неврологический журнал Том 21, №1, 2025
Вернуться к номеру
Дослідження впливу субтотальної резекції на виживаність при гліобластомі: клінічний випадок
Авторы: Dipak Chaulagain, V. Smolanka, A. Smolanka, T. Havryliv
Regional Clinical Center of Neurosurgery and Neurology, Uzhhorod National University, Uzhhorod, Ukraine
Рубрики: Неврология
Разделы: Справочник специалиста
Версия для печати
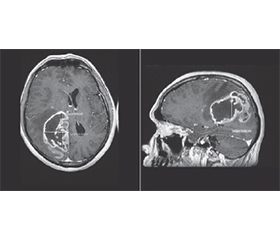
Гліобластома, що характеризується агресивним перебігом і поганим прогнозом, залишається складною проблемою нейроонкології. Стандартні методи лікування, включно з максимально безпечною хірургічною резекцію, подальшою ад’ювантною хіміотерапією та променевою терапією, спрямовані на продовження життя й полегшення симптомів. Однак, незважаючи на ці втручання, прогноз залишається несприятливим, особливо за субтотальної резекції. У цьому клінічному випадку розглядається вплив субтотальної резекції на виживаність пацієнтів із гліобластомою. 46-річний чоловік звернувся зі скаргами на головний біль і слабкість лівої сторони тіла, що потребувало госпіталізації та подальшого хірургічного втручання. Проведено субтотальну резекцію з видаленням приблизно 95 % пухлини. Після операції пацієнт отримував хіміотерапію темозоломідом (75 мг/м2) протягом шести тижнів, але від променевої терапії відмовився. Примітно, що після лікування чоловік відчув полегшення симптомів і прожив шість місяців. Цей клінічний випадок підкреслює потенціал субтотальної резекції в лікуванні гліобластоми, особливо у випадках, коли повне видалення пухлини неможливо. Також наголошується на важливості індивідуального підходу до лікування й необхідності подальших досліджень для оптимізації результатів у пацієнтів із гліобластомою, які мають менш сприятливий прогноз.
Glioblastoma characterized by aggressive nature and poor prognosis remains a challenging entity in neuro-oncology. Standard treatment modalities, including maximal safe surgical resection followed by adjuvant chemotherapy and radiotherapy, aim to prolong survival and alleviate symptoms. However, despite these interventions, prognosis remains dismal, particularly in cases of subtotal resection. This case study delves into the effect of subtotal resection on survival outcomes in glioblastoma patients. A 46-year-old male presented with symptoms of headache and left-sided weakness, prompting admission and subsequent surgical intervention. Subtotal resection, achieving approximately 95 % tumor removal, was performed. Following surgery, the patient underwent chemotherapy with temozolomide (75 mg/m2) for six weeks, omitting radiotherapy. Remarkably, the patient experienced symptom alleviation post-treatment and survived for six months. This case highlights the potential of subtotal resection in managing glioblastoma, particularly in cases where complete excision is not feasible. Additionally, it underscores the need for individualized treatment approaches and further research to optimize outcomes in glioblastoma patients with less favorable prognoses.
гліобластома; субтотальна резекція; обсяг резекції; результат виживання
glioblastoma; subtotal resection; extent of resection; survival outcome