
Журнал «Почки» Том 14, №1, 2025
Вернуться к номеру
Стратегія виходу після черезшкірної нефролітотомії: вплив розміру трубки на раннє видалення порівняно з бездренажною черезшкірною нефролітотомією — дебати тривають
Авторы: Ihab S. Khewkah (1), Raed H. Afiet (2), Haidar H. Al Jabban (1)
(1) - Alyarmook Teaching Hospital, Urology Department, Baghdad, Iraq
(2) - Medical City Complex, Surgical Specialties Hospital, Urology Department, Baghdad, Iraq
Рубрики: Нефрология
Разделы: Клинические исследования
Версия для печати
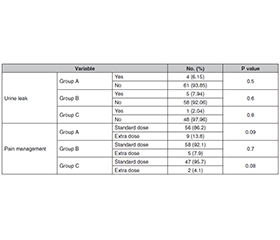
Актуальність. Багато досліджень, у яких намагалися уникнути встановлення нефростомічної трубки (НТ), щоб зменшити дискомфорт пацієнта та скоротити перебування в лікарні, продемонстрували ефективність і безпеку бездренажної та повністю бездренажної черезшкірної нефролітотомії (ЧШНЛ). Однак, враховуючи, що нефростомічна трубка слугує резервним планом безпеки при небажаних подіях, як-от залишковий камінь та інтраопераційна кровотеча, варто розглянути інший розмір трубки, якщо ми хочемо подолати ніч (раннє видалення трубки), і порівняти цей варіант із бездренажною ЧШНЛ. Мета: оцінити вплив розміру трубки (при ранньому видаленні) на післяопераційний перебіг порівняно з бездренажною ЧШНЛ. Матеріали та методи. У період з грудня 2020 р. по червень 2022 р. 177 пацієнтів із сечокам’яною хворобою були відібрані для проходження ЧШНЛ та перебували під проспективним спостереженням. Наприкінці процедури вони були випадковим чином розподілені на 3 групи. Група A — з розміщенням НТ розміром 18Fr, група В — НТ розміром 8Fr і група С — без нефростоми. У групах А і В нефростому залишали на одну добу. У групі C застосовувалося ручне стиснення бокової ділянки протягом декількох хвилин, а прокол шкіри був закритий одним швом. Групи порівнювали щодо післяопераційного зниження рівня гематокриту, витоку сечі, потреби в додатковому знеболюванні та будь-яких інших післяопераційних подій. Результати. Чоловіків було 52,3; 58,7 і 55,1 % у групах A, B і C відповідно. Тривалість гематурії становила 6,28 ± 2,94 години для групи А, 8,80 ± 3,45 години для групи В і 13,67 ± 2,40 години для групи С. У той же час середнє післяопераційне зниження рівня гематокриту у групі A дорівнювало 0,60 ± 0,14 мг/дл, у групі В — 0,82 ± 0,20 мг/дл та 1,33 ± 0,25 мг/дл у групі C (p < 0,001). Висновки. НТ великого діаметра протягом короткого періоду (одна доба) забезпечує чудовий контроль кровотечі, витоку сечі та післяопераційної потреби в аналгетиках, порівнянний з таким при використанні НТ малого діаметра та режиму без НТ. Це також зберігає можливість повторної нефроскопії, якщо це необхідно.
Background. Many studies have demonstrated the efficacy and safety of tubeless and totally tubeless percutaneous nephrolithotomy (PCNL), trying to avoid putting a nephrostomy tube (NT) to decrease patient discomfort and shorten hospital stay. However, given that nephrostomy tube serves a safety backup plan for adverse events like residual stone and intraoperative bleeding, it is worth investigating different tube size if we want to bridge the night (early tube removal) and compare it to tubeless PCNL. The purpose was to evaluate the effect of tube size (with early removal) on postoperative course compared to NT free. Materials and methods. During the period from December 2020 to June 2022, 177 patients with renal stones were selected to undergo PCNL and were prospectively followed up. At the end of procedure, the patients were randomly distributed into 3 groups. Group A, those with placement of an 18Fr NT, group B, those with placement of an 8Fr tube and group C, nephrostomy-free. For group A and B, the nephrostomy was left in place for 1 day. For group C, manual compression was applied to the flank for few minutes and the skin puncture was closed with one stitch. The groups were compared for post-operative hematocrit drop, urine leakage, need for additional analgesia and any other postoperative events. Results. The mean age for group A was 34.110 ± 6.919 years, group B was 38.670 ± 9.935 years and group C was 37.270 ± 10.657 years (F = 3.567, p = 0.03). The post hoc Tukey analysis showed a significant difference between groups A and B (p = 0.036), however, no differences were recorded between groups A and C (p = 0.203) or B to C (p = 0.714). The present study showed that the mean stone burden was 34.03 ± 5.40 mm for group A, 33.43 ± 5.60 mm for group B and 33.43 ± 4.90 mm for group C, with no significant differences (p = 0.773). The post hoc Tukey analysis showed no significant difference between groups A and B (p = 0.818), A and C (p = 0.815), B and C (p = 0.857). The male percentage was 52.3, 58.7 and 55.1 % for group A, B and C, respectively. In this study, the duration of hematuria was 6.28 ± 2.94 hours for group A, 8.80 ± 3.45 hours for group B and 13.67 ± 2.40 hours for group C, these results were statistically significant (p < 0.0001). The post hoc Tukey analysis showed a significant difference between groups A and B (p = 0.0002), A and C (p = 0.0000), groups B and C (p = 0.0000). In the current study, the mean postoperative hematocrit drop for group A was 0.60 ± 0.14 mg/dl, 0.82 ± 0.20 mg/dl for group B and 1.33 ± 0.25 mg/dl for group C. These results were statistically significant (p < 0.0001). The post hoc Tukey analysis showed a significant difference between groups A and B (p = 0.0002), A and C (p = 0.0000), groups B and C (p = 0.0000). Conclusions. Large bore NT (18Fr) for short duration (one day) provide superior bleeding control and comparable postoperative analgesic requirement and urine leak when compared to small bore NT (8Fr) and NT free. It also keeps the chance for second look nephroscopy if needed.
стратегія виходу; черезшкірна нефролітотомія; розмір нефростомічної трубки; бездренажна процедура
exit strategy; percutaneous nephrolithotomy; nephrostomy tube size; tubeless
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Bolton D, Hennessey D. Exit strategies after percutaneous nephrolithotomy. In: Smith AD, Preminger GM, Kavoussi LR, Badlani GH, Rastinehad AR, eds. Smith’s Textbook of Endourology. 1st ed. New York: John Wiley & Sons Ltd; 2018. 427-440. Available from: https://onlinelibrary.wiley.com/doi/book/10.1002/9781119245193.
- Ichaoui H, Samet A, Ben Hadjalouane H, Hermi A, Hedhli H, et al. Percutaneous nephrolithotomy (PCNL): Standard technique versus tubeless — 125 procedures. Cureus. 2019 Mar 14;11(3):e4251. doi: 10.7759/cureus.4251.
- Wilhelm K, Hein S, Kunath F, Schoenthaler M, Schmidt S. Totally tubeless, tubeless, and tubed percutaneous nephrolithotomy for treating kidney stones. Cochrane Database Syst Rev. 2023 Jul 28;7(7):CD012607. doi: 10.1002/14651858.CD012607.pub2.
- Zeng GH, Zhong W, Mazzon G, Zhu W, Lahme S, et al. International Alliance of Urolithiasis (IAU) consensus on miniaturized percutaneous nephrolithotomy. Mil Med Res. 2024 Oct 28;11(1):70. doi: 10.1186/s40779-024-00562-3.
- Iqbal N, Iqbal S, Hasan A, Iqbal A, Blair KAA, Milstein DMJ, Akhter S. Outcome of tubeless percutaneous nephrolithotomy in elder patients: A single-center experience from a developing country. J Clin Transl Res. 2022 Mar 19;8(2):160-165.
- Nikoufar P, Hodhod A, Hadi RA, Abbas L, Vangala SK, et al. Safety and efficacy of ambulatory tubeless mini-percutaneous nephrolithotomy in the management of 10–25 mm renal calculi: A retrospective study. Can Urol Assoc J. 2024 Oct;18(10):341-347. doi: 10.5489/cuaj.8764.
- Zhao Z, Yin S, Zhu H, Cheng D, Liu Y, Zeng G. The feasibility of multiple-tract mini-percutaneous nephrolithotomy as an overnight surgery for the treatment of complex kidney stones. Urolithiasis. 2021 Apr;49(2):167-172. doi: 10.1007/s00240-020-01208-4.
- Lin CH, Lin YC, Chiang HC, Yan MY, Fang WY, Chen PH. Totally tubeless single access tract mini-percutaneous nephrolithotripsy in treatment of large burden > 2-cm and/or complex renal stones: A case series of 62 patients. BMC Urol. 2022 Apr 16;22(1):61. doi: 10.1186/s12894-022-01012-9.
- Li Q, Gao L, Li J, Zhang Y, Jiang Q. Total tubeless versus standard percutaneous nephrolithotomy: A meta-analysis. Minim Invasive Ther Allied Technol. 2019;29(2):61-69. doi: 10.1080/13645706.2019.1581224.
- Abdelgawad E, Kadry AM, Abdelhalim KM, Abdelwahab HA. Optimization of the outcome of percutaneous nephrolithotomy regarding urinary leakage: What should we do? Urolithiasis. 2022 Dec 2;51(1):8. doi: 10.1007/s00240-022-01375-6.
- Chen T, Zhu Z, Du J. Efficacy of intercostal nerve block for pain control after percutaneous nephrolithotomy: A systematic review and meta-analysis. Front Surg. 2021 Jan 28;8:623605. doi: 10.3389/fsurg.2021.623605.
- Poudyal S. Current insights on hemorrhagic complications in percutaneous nephrolithotomy. Asian J Urol. 2022 Jan;9(1):81-93. doi: 10.1016/j.ajur.2021.05.007.
- Luo Y, Camey SA, Bangdiwala SI, Palsson OS, Sperber AD, Keefer LA. Global patterns of prescription pain medication usage in disorders of gut-brain interactions. Neurogastroenterol Motil. 2023 Jan;35(1):e14457. doi: 10.1111/nmo.14457.
- Cormio L, Preminger G, Saussine C, Buchholz N, Zhang X, Walfridsson H, et al. Nephrostomy in percutaneous nephrolithotomy (PCNL): Does nephrostomy tube size matter? Results from The Global PCNL Study from The Clinical Research Office Endourology Society. World J Urol. 2012;31(6):1563-1568. doi: 10.1007/s00345-012-0969-z.
- Bhat S, Lal J, Paul F. A randomized controlled study compa–ring the standard, tubeless, and totally tubeless percutaneous nephrolithotomy procedures for renal stones from a tertiary care hospital. Indian J Urol. 2017 Oct-Dec;33(4):310-314. doi: 10.4103/iju.IJU_52_17.