
Журнал «Травма» Том 26, №3, 2025
Вернуться к номеру
Моделювання роботи м’язів при згинанні верхньої кінцівки в плечовому суглобі
Авторы: Кравченко Д.Д. (1, 2), Страфун О.С. (2), Суворов В.Л. (2), Карпінська О.Д. (3), Карпінський М.Ю. (3)
(1) - ДНУ «Центр інноваційних медичних технологій НАН України», м. Київ, Україна
(2) - ДУ «Інститут травматології та ортопедії НАМН України», м. Київ, Україна
(3) - ДУ «Інститут патології хребта та суглобів імені професора М.І. Ситенка НАМН України», м. Харків, Україна
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
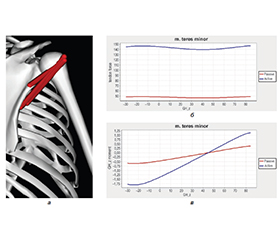
Актуальність. Процедура ендопротезування часто застосовується при переломах або масивних розривах м’язів ротаторної манжети, коли консервативне лікування неефективне. У випадках, коли неможливо застосовувати анатомічне ендопротезування плечового суглоба, широко використовується реверсивне ендопротезування. При заміщенні плечового суглоба важливо враховувати внесок м’язів, відповідальних за згинання та відведення плеча, оскільки їхня функція суттєво впливає на стабільність протеза, діапазон рухів і загальну ефективність відновлення. Мета: оцінити силовий внесок окремих м’язових груп при згинанні верхньої кінцівки в плечовому суглобі для подальшого застосування в біомеханіці та клінічній практиці. Матеріали та методи. У структуру моделі входять 6 суглобових з’єднань: надплечово-ключичне (аrticulatio acrimio-clavicularis), грудинно-ключичне (аrticulatio sternoclavicularis), плечове (articulatio glenohumeralis), плечоліктьове (аrticulatio humeroulnaris), плечо-променеве (аrticulatio humeroradialis) та променево-зап’ясткове (аrticulatio radiocarpalis). Розглядали рух верхньої кінцівки без навантаження (рassive) та при згинанні з вагою 2 кг. Результати. При пасивних рухах м’язи-ротатори манжети плеча виконують переважно пасивну роль стабілізаторів і до кута 30–40° не збільшують силу стабілізації. Але при згинанні руки з вагою 2 кг відмічається збільшення активації м’язів, причому м’язи, розташовані зверху (m. supraspinatus), активуються помітно менше, приблизно удвічі, на відміну від бічних м’язів (m. subscapular, m. infraspinatus і m. teres minor), сила яких збільшується втричі. Це пов’язано з тим, що верхній м’яз (m. supraspinatus) при згинанні руки не змінює вектор дії сил, більш того, у міру збільшення кута згинання зменшується його довжина, що і зменшує необхідну силу. Тобто основна його роль у підтримці стабільності суглоба — утримання голівки плеча. М’язи, розташовані з боку лопатки, при зміні кута згинання, крім зміни векторів дії сили, збільшують свою довжину, хоча і незначно, але в силу дії гравітаційних сил при згинанні руки з вагою для підтримки стабільності плеча м’язи збільшують свою силу. Згинання руки до 40–60° відбувається переважно рухами у плечовому суглобі (гленоїді), який забезпечується передньою порцією дельтоподібного м’яза, великим грудним м’язом і безпосередньо біцепсом. Подальший рух потребує задіяння м’язів, відповідальних за рух лопатки (m. serratus anterior, m. trapezius (pars descendens), mm. rhomboidei). При ендопротезуванні плечового суглоба за можливості бажано зберегти м’язи ротаторної манжети плеча і дельтоподібний м’яз або домагатися мінімального їх ушкодження. M. teres minor, як частина ротаторної манжети, разом з m. infraspinatus утримує суглоб, запобігаючи вивиху протеза. Дельтоподібний м’яз і манжета (включно з teres minor) забезпечують флексію, ротацію та відведення. Пошкодження веде до слабкості, втрати зовнішньої ротації та ускладнень (наприклад, нестабільності). Висновки. Отримані результати моделювання підтверджують, що м’язи ротаторної манжети плеча в основному відіграють роль у стабілізації плечового суглоба. У пасивному режимі (без ваги) вони проявляють мінімальну активність до кута згинання 30–40°, виконуючи переважно пасивну стабілізаційну функцію. Натомість при згинанні руки з додатковою вагою спостерігається значне зростання сили м’язів-стабілізаторів, що свідчить про їх активну участь у протидії гравітаційному навантаженню та утриманні головки плечової кістки. Отримані дані є цінними при плануванні ендопротезування плечового суглоба. Збереження м’язів ротаторної манжети має вирішальне значення для забезпечення стабільності протеза, рухливості суглоба та запобігання післяопераційним ускладненням.
Background. The endoprosthetic procedure is often used for fractures or massive ruptures of the rotator cuff muscles, when conservative treatment is ineffective. In cases where it is impossible to use anatomical shoulder replacement, reversible arthroplasty is widely used. When replacing the shoulder joint, it is important to consider the contribution of the muscles responsible for flexion and abduction of the shoulder, since their function significantly affects the stability of the prosthesis, range of motion and overall recovery efficiency. Objective: to assess the force contribution of individual muscle groups during flexion of the upper limb in the shoulder joint for further use in biomechanics and clinical practice. Materials and methods. The structure of the model includes 6 joints: acromioclavicular (articulatio acromioclavicularis), sternoclavicular (articulatio sternoclavicularis), humeral (articulatio glenohumeralis), humeroulnar (articulatio humeroulnaris), humeroradial (articulatio humeroradialis) and radiocarpal (articulatio radiocarpalis). We considered the movement of the upper limb without load (passive) and when bending with a weight of 2 kg. Results. During passive movements, the rotator cuff muscles perform a predominantly passive role of stabilizers and do not increase the stabilization force with an angle of up to 30–40°. However, when bending the arm with a weight of 2 kg, an increase in muscle activation is noted, and the muscles located above (m. supraspinatus) are activated noticeably less, about 2-fold, unlike the lateral muscles (m. subscapularis, m. infraspinatus and m. teres minor), whose strength increases threefold. This is due to the fact that the upper muscle (m. supraspinatus) does not change the vector of force action when bending the arm; moreover, as the bending angle increases, its length decreases, which reduces the required force. That is, its main role in maintaining joint stability is holding the shoulder head. The muscles located on the side of the scapula, when changing the angle of flexion, in addition to changing the force vectors, increase their length, although not significantly, but due to the action of gravitational forces, when bending the arm with weight, to maintain the stability of the shoulder, the muscles increase their strength. Flexion of the arm to 40–60° occurs mainly by movements in the shoulder joint (glenoid), which is provided by the anterior portion of the deltoid muscle, the pectoralis major muscle and directly the biceps. Further movement requires the involvement of the muscles responsible for the movement of the scapula (m. serratus anterior, m. trapezius (pars descendens), mm. rhomboidei). In shoulder replacement, if possible, it is desirable to preserve the rotator cuff muscles and the deltoid muscle or try to damage them minimally. The teres minor muscle as part of the rotator cuff, together with the infraspinatus muscle holds the joint, preventing dislocation of the prosthesis. The deltoid muscle and the cuff (including the teres minor) provide flexion, rotation, and abduction. Damage leads to weakness, loss of external rotation, and complications (e.g., instability). Conclusions. The modeling results confirm that the rotator cuff muscles mainly play a role in stabilizing the shoulder joint. In the passive mode (without weight), they show minimal activity up to a flexion angle of 30–40°, performing a predominantly passive stabilization function. In contrast, when the arm is flexed with additional weight, there is a significant increase in the strength of the stabilizer muscles, which indicates their active participation in counteracting the gravitational load and holding the humeral head. The data obtained are valuable in planning shoulder arthroplasty. Preservation of the rotator cuff muscles is crucial for ensuring prosthesis stability, joint mobility, and preventing postoperative complications.
плечовий суглоб; згинання; м’язи; ізометрична сила; момент сили
shoulder joint; flexion; muscles; isometric force; moment of force