
Журнал «Травма» Том 26, №3, 2025
Вернуться к номеру
Дослідження напружено-деформованого стану моделі стегнової кістки з ревізійною ніжкою після розширеної проксимальної остеотомії залежно від варіантів фіксації кісткового клаптя серкляжним дротом
Авторы: Бондаренко С.Є., Філіпенко В.А., Олінкевич Є.В., Марущак О.П., Карпінський М.Ю., Яресько О.В.
ДУ «Інститут патології хребта та суглобів імені професора М.І. Ситенка НАМН України», м. Харків, Україна
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
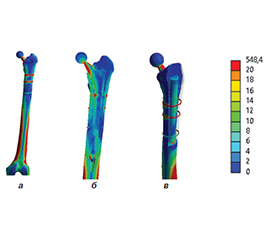
Актуальність. Однією з проблем при ревізійному ендопротезуванні кульшового суглоба є видалення стабільного стегнового компонента. Використання серкляжного дроту для фіксації кісткового клаптя після остеотомії має кілька невирішених питань, що стосуються вибору оптимальної кількості рівнів фіксації остеотомованого клаптя, обертів серкляжного дроту та ступеня післяопераційного навантаження на прооперовану нижню кінцівку. Мета: провести порівняльний аналіз величин напружень в моделі стегнової кістки з ревізійною ніжкою після розширеної проксимальної остеотомії (еxtended trochanteric osteotomy, ETO) залежно від варіантів фіксації кісткового клаптя серкляжним дротом. Матеріали та методи. Розроблена базова скінченно-елементна модель стегнової кістки з ревізійним ендопротезом. Модель містила стегнову кістку, ревізійний ендопротез, кістковий клапть. Моделювали три варіанти фіксації кісткового клаптя на одному, двох та трьох рівнях. На кожному рівні накладали по 2 витки серкляжного дроту діаметром 1,5 мм. Модель навантажували розподіленою силою величиною 1100 Н. Результати. При фіксації кісткового клаптя на одному рівні максимальні напруження в стегновій кістці визначаються на дистальній частині її діафіза — 48,1 та 43,9 МПа відповідно з медіального та латерального боків. Мінімальний рівень напружень 8,7 МПа визначено в кістковому клапті, що пояснюється наявністю між ним та стегновою кісткою міжуламкового регенерату, який виконує демпфуючу функцію. Напруження в ендопротезі мають тенденцію до зростання від 158,8 МПа в шийці до 213,4 МПа на проксимальному кінці ніжки. Максимум рівня напружень 834,1 МПа спостерігається в серкляжному дроті, що в 1,6 раза перевищує межу міцності хірургічної сталі і може стати причиною розриву дроту. Фіксація кісткового клаптя серкляжним дротом на двох рівнях призводить до зниження величин напружень у всіх контрольних точках на стегновій кістці. Зниження величин напружень у 2 рази визначене в серкляжному дроті, що пов’язано з перерозподілом навантажень на дві точки фіксації. Дротова обмотка на третьому рівні практично не відобразилася на розподілі напружень в кісткових елементах моделі. Висновки. Фіксація кісткового клаптя на двох та трьох рівнях суттєво не впливає на рівень напружень у стегновій кістці, але дозволяє вдвічі знизити величину напружень в самому дроті, який при однорівневій фіксації може перевищувати межу міцності хірургічної сталі. У разі технічно відсутньої можливості виконання фіксації на декількох рівнях може бути використана однорівнева фіксація за умов використання намотки дроту не менш ніж 4 оберти та навантаження на оперовану кінцівку не більше 50 %. Оптимальним варіантом фіксації кісткового клаптя є дворівнева серкляжна фіксація, яка забезпечує зниження напружень у дроті нижче межі міцності хірургічної сталі. Трирівнева фіксація забезпечує ще більше зниження напружень у дроті до 326,2 МПа, але різниця порівняно з дворівневою фіксацією не є настільки суттєвою, щоб виправдати додаткову травматизацію тканин та подовження часу операції. Обмеження навантаження на оперовану кінцівку до 50 % дозволяє знизити напруження в серкляжному дроті нижче критичних значень навіть при однорівневій фіксації, що може бути рекомендовано для раннього післяопераційного періоду до формування достатньо міцного міжуламкового регенерату.
Background. One of the problems in revision hip arthroplasty is the removal of the stable femoral component. The use of a cerclage wire for fixing the bone flap after osteotomy raises several unresolved issues: the choice of the optimal number of the osteotomized flap fixation levels, the number of cerclage wire turns, and the degree of postoperative load on the operated lower limb. The purpose was to conduct a comparative analysis of the stress values in the femoral model with a revision stem after extended proximal osteotomy (ETO) depending on the options for fixing the bone flap with a cerclage wire. Materials and methods. A basic finite element model of the femur with a revision endoprosthesis was created. It contained femur, revision endoprosthesis, and bone flap. Three options for fixing the bone flap at one, two, and three levels were modeled. Two turns of a cerclage wire with a diameter of 1.5 mm were applied at each level. The model was loaded with a distributed force of 1100 N. Results. When fixing the bone flap at one level, the maximum stresses in the femur are determined at the distal part of its diaphysis — 48.1 and 43.9 MPa, respectively, from the medial and lateral sides. The minimum stress level of 8.7 MPa was revealed in the bone flap, which is explained by the presence of interfragmentary regenerate between it and the femur, which performs a damping function. Stresses in the endoprosthesis tend to increase from 158.8 MPa in the neck to 213.4 MPa at the proximal end of the stem. The maximum stress level of 834.1 MPa is observed in a cerclage wire, which is 1.6 times higher than the tensile strength of surgical steel and can cause wire breakage. Fixation of the bone flap with a cerclage wire at two levels leads to a decrease in stress values at all control points on the femur. A decrease in stress values by 2 times was determined in a cerclage wire, which is associated with the redistribution of loads to two fixation points. The wire winding at the third level practically didn’t influence the stress distribution in the bone elements of the model. Conclusions. Fixation of the bone flap at two and three levels does not significantly affect stresses in the femur but allows you to halve the magnitude of stress in the wire itself, which with a single-level fixation can exceed the tensile strength of surgical steel. In the absence of technical possibilities to perform fixation at several levels, a single-level fixation can be applied under the conditions of using a wire winding of at least 4 turns and a load on the operated limb of no more than 50 %. The optimal option for fixing the bone flap is a two-level cerclage fixation, which provides a reduction in stresses in the wire below the tensile strength of surgical steel. Although a three-level fixation provides an even greater reduction in stresses in the wire to 326.2 MPa, the difference compared to a two-level fixation is not so significant as to justify additional tissue trauma and extending the operation time. Limiting the load on the operated limb to 50 % allows reducing the tension in a cerclage wire below critical values even with a single-level fixation, which can be recommended for the early postoperative period until a sufficiently strong interfragmentary regenerate is formed.
кульшовий суглоб; ревізійне ендопротезування; розширена проксимальна остеотомія
hip joint; revision arthroplasty; extended proximal osteotomy